
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Anna Hudáková*, Ľudmila Majerníková and Štefánia Andraščíková
Corresponding Author: Anna Hudáková, University of Presov in Presov, Faculty of Health Care, Department of Nursing, Presov, Slovakia.
Received: March 17, 2023 ; Revised: April 02, 2023 ; Accepted: April 05, 2023 ; Available Online: April 20, 2023
Citation: Hudáková A, Majerníková L & Andraščíková S. (2023) Implementation of Methods of Measuring the Quality of Life in Nursing. J Nurs Midwifery Res, 2(1): 1-5.
Copyrights: ©2023 Hudáková A, Majerníková L & Andraščíková S. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
Objectives: The main objective of this study was to analyze the perception of subjective and objective quality of life among our respondents. We wanted to determine which of the methods used by nurses in clinical practice and highlight the individual domains that respondents considered most important in assessing the overall quality of life.
Methods: The research was conducted in the form of a questionnaire, the research sample consisted of 155 respondents-nurses working in the General Hospital and Policlinic Levoca. The statistical processing of the results, we used the Mann-Whitney test, Chi-square test, Student's t-test and interval estimation of the average.
Results: Based on the statistical processing of data, we found significant differences in perception between subjective and objective quality of life for our respondent (p-0.001). The Scale of life meaningfulness was known to 17.1% of university-educated nurses and 25% of secondary educated nurses, there weren’t significant differences between the selected group of respondents (p-0.237). Quality of Life Enjoyment and Satisfaction Questionnaire) is known by 71.4% of nurses. There are significant differences in the examined area of knowledge of the nurses and their completed education (p-0.001).
Conclusion: From the results of the research, we found that nurses know only certain methods for measuring the quality-of-life suring quality of life in nursing. The methods for measuring quality of life in nursing major contribution to nursing practice, because it allows detection of many problems in patients.
Keywords: Nurses, Clinical practice, Methods, Quality of life, Education
INTRODUCTION
The concept of quality of life as a priority assumes that the social and physical environment affects the QoL of the people living in it. The process of perception can be understood as a series of physiological, social and psychological factors that are responsible for feeling (dis) satisfaction with the environment that surrounds an individual or social group [1]. Health is now seen as a “metasystem” comprised of various interconnected systems; physical, mental and social, and it depends on how a person or social group perceives and interprets health and disease, how it responds to ideas about the human body and its functioning [2]. The concept of health itself is defined as the “dynamic equilibrium of the body in relation to endogenous and exogenous conditions that will ensure its proper functioning”. The society-wide importance of health today is perceived not only as a social indicator of quality of life but also as a factor which is of growing importance as a source for social and economic development of the regions [3]. Evaluation tools that try to capture the objective state of physical health of individuals and their satisfaction with health are sufficiently sophisticated. Gurková, Žiaková [4] define the quality of life through three approaches: psychological, applicational and synthesizing. The psychological approach focuses on conceptual differentiation between the concepts of quality of life, well-being and satisfaction. When evaluating the applicational approaches to quality of life, they point to the difference between concepts such as: health, health condition, quality of life. When processing synthesizing approaches, they integrated components and factors of quality of life into the same theoretical framework, based on conceptual models. Ondrejka [5] says that the concept of quality of life should express the complex, subjective and dynamically changing the status of the individual, and should therefore be multidimensional, each component should be determined multifactorial. The concept of health-related quality of life (HRQoL) is found in many electronic databases and has multiple instruments. Proof of this is the tool developed by a working group and in cooperation with the WHO which is known as WHOQOL (World Health Organization Quality of Life). It incorporates the perception of quality of life from a subjective point of view and in conjunction with daily activities [6]. The consensus of opinion that prevails in nursing considers quality of life to be a subjective phenomenon. Quality of life is defined as the subjective perception and evaluation. Haase, Braden [7] draws attention of the conceptual confusion that arose in defining objective and subjective quality of life. These are mainly due to imprecise use of terms such as: subjective quality of life versus the subjective well-being, subjective quality of life versus satisfaction, satisfaction versus subjective well-being, objective quality of life versus functional status. The author emphasizes that the concepts of subjective well-being, satisfaction and functional status should not be equated with the concept of quality of life [8]. Distinguishes between short emotional episodes, feelings of joy or happiness and momentary nature of the state of happiness, which is designed as a feeling of satisfaction in specific areas of an individual's life such as relationships work and health.
MATERIAL AND METHODS
We wanted to analyze the perception of subjective and objective quality of life among our respondents in terms of their education and satisfaction with health. In this paper we investigated the level of knowledge of nurses in methods to measure of areas quality of life in nursing. We wanted to see which methods nurses use in clinical practice. The research sample consisted of 155 nurses working in the General Hospital and Policlinic Levoca. The dependent variables consisted of the level of knowledge of methods to measure the quality of life in nursing, knowledge of the individual scales for monitoring quality of life, which are used in clinical practice and the attitudes of nurses to the use of methods for measuring quality of life in clinical practice. The independent variable was the education of the respondents. The statistical processing of the results, we used the Mann-Whitney test, Chi-square test, Student's t-test and interval estimation of the average.
RESULTS
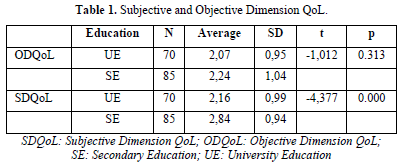
We can examine quality of life at different levels and spheres ranging from the macro level, through the national level or as a specification of the quality of life for individual selected groups. At present there is now an indisputable duality of QoL or 2-dimensiality to the stated concept (Table 1). The main dimension is the preferred subjective-psychological dimension, dealing with how individuals live their life (human wellbeing). The second researched dimension is the dimension is the objective-spatial one analyzing in particular the conditions in which people live their lives (Environmental Quality) [2].
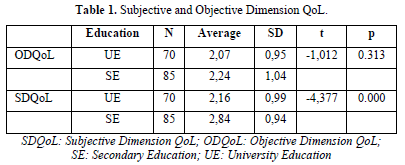
We expected that there is a statistically significant relationship between the perception of subjective and objective quality of life in our nurses. On the basis of the correlation coefficient (p=0.001) we found that the more positive view of nurses of their objective quality of life (physical health, material security, social status in the society), the more positive their assessments of their subjective quality of life (human emotionality, general satisfaction with life). Significant differences in the perception of the quality of life and satisfaction with health were verified using the Mann-Whitney U test. In finding the perception of overall quality of life in nurses was found positive statistical significance (p=0.034). Within the area of educational attainment, nurses with secondary education more satisfied with their health compared with nurses with higher education, who assessed the quality of their health as “average”. The results of the Mann-Whitney U test (p=0.002) confirmed that there is a relationship between the ordinal variable and the binary variable (Table 2).

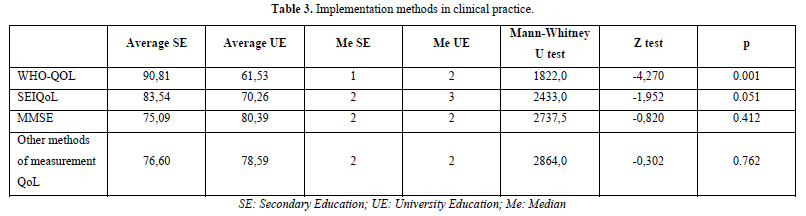
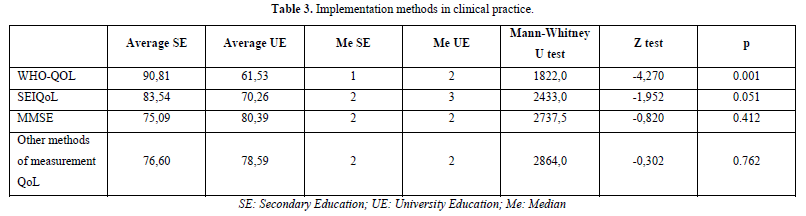
To verify the perception of satisfaction with life in the research sample hypothesis we used the Chi-square test of conformance of distribution. We assumed that over 50% of our nurses will indicate positive responses (to be a “generally” satisfied with their lives). From an overall analysis of the results of research we assess that they are satisfied with their lives (p=0.001). Personal perception of the quality of life of respondents assumes the boiling down of one’s own opinions into to the individual subscales evaluating quality of life, and then the possible use of methods and measurements of quality of life in practice. Attempts to quantification it in any ways must be preceded by an overall operationalization of all concepts as well as the choice of specific indicators of quality of life. The indicators produce a whole series of functions. They can simplify and clarify aggregated information for decision making while helping to integrate the natural and social sciences in decision making and moving towards sustainable development. Indicators are important tools for the transfer of ideas and values. Evaluation and monitoring of QoL through a variety of indicators is addressed by a range of global programs and institutions. In this regard, they are increasingly beginning to discover and also make use of aggregated indicators of QoL [9]. We expected that there are significant differences in the research sample in terms of knowledge of elementary methods for measure selected areas quality of life that are used in their practice. Also, we expected that respondents had more fully encountered at least two methods for measuring quality of life. This hypothesis was verified using the Mann-Whitney U test, Chi-square test for conformity of distributions and Z test. The nurses confirmed that in their practice at the hospital, possibly during training, they had encountered a standard type of questionnaire to assess quality of life as WHOQOL (p=0.001). Nurses in our sample had only occasionally encountered the SEIQoL (Schedule for the Evaluation of Individual Quality of Life) method of measuring the quality of life through a questionnaire, which assesses twelve categories of life goals (p=0.051). The SEIQoL method was created by the combination of the two methods: Daily reports mood and Diener´s methods. They investigating the extent to which we are able to accomplish set goals in life. The Diener method includes the results of the factor analysis of some adjectives that describe the mood of an individual [10]. Among the ways to measure individual satisfaction with life and its overall quality is the method Daily mood reports. That method requires a person to record their feelings at regular time intervals (Table 3).
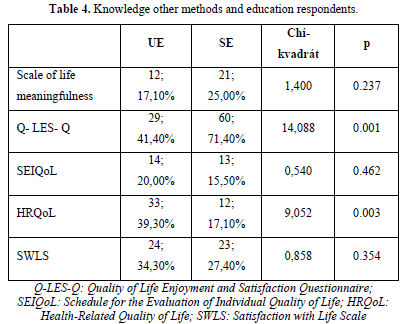
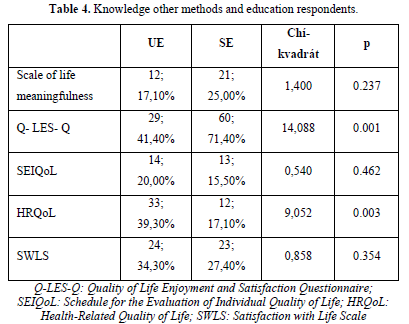
The Scale of life meaningfulness [11] was known to 17.1% of university-educated nurses and 25% of secondary educated nurses. There weren’t significant differences between the selected groups of respondents (p=0.237). The scale of life meaningfulness consists of twenty statements relating to the respondent's life and are marked on a scale from 1 (strongly disagree) to 5 (strongly agree). The cognitive dimension includes items related to overall life direction, mission in life and understanding of life. The motivational dimension is made up of items including goals, objectives, and motivation at the same time as engagement in them. Affective dimension consists of items comprising life satisfaction, optimism; fulfilment put also includes a feeling of monotony, a feeling of disgust. The interview of life joy and satisfaction Q-LES-Q (Quality of Life Enjoyment and Satisfaction Questionnaire) is known by 71.4% of nurses. There are significant differences in the examined area of knowledge of the nurses and their completed education (p=0.001). When using the HRQoL method, statistical significance (p=0.003) was confirmed in favor of nurses UE (39.30%) compared to nurses SE (1710%) (Table 4).
Social support has significant influence on the evaluation of quality of life. We evaluated the effect of social support on the overall perception of life of nurses. We investigated what domains are preferred for nurses for evaluation of quality of life. There was no statistically significant relationship between a selected group of nurses. Nurses perceive social support as help with the active support of close persons participating in dealing with stressful situation. In terms of social support, we must consider not only the right timing, but also the necessary level of social support that we provide to the client. A very low level of social support, but also an excessively high level may paradoxically lead to a reduction in the ability to handle challenging situations.
DISCUSSION
In terms of perception of the concept of quality of life, both groups’ nurses consider the less important to be physical domain (p=0.161). Waterman [12] provides a conceptual model for grasping and subsequent measurement of QoL in time, which implies that in the perception of the individual, there occurs some shift to so-called. “Response shift”. To accelerate the course of the shift, the first dimension is involved which is covered by the model “catalyst for change”, which can change the health of individuals. The second dimension consists of socio-demographic characteristics, characterized by age, sex and some stable characteristics of personality (optimism, expectations, spiritual integration). The third dimension of the model are the cognitive, behavioral and emotional processes that produce “Mechanisms of change” through which individuals try to adapt to their changing condition. The above mechanism includes individual coping strategies, social comparison, changes in the hierarchy of objectives and expectations of the individual. The fourth dimension of the model is “The shift in response,” which affects the individual's sense of evaluation and QoL. The result of this change is recalibration thereby changing the internal standards and individual programmes on the scale of values, a change in the hierarchy of values and change of concepts- reconceptualization [13]. The perceived quality of life is the final dimension of the model, consisting of physical, psychological and social fields, a multidimensional construct. Mareš [14] states the process QoL model who examined individual transformations occurring under the influence of certain external events and the internal changes taking place in a person. Under that model was to examined changes in the quality of life of women after diagnosis and initiation of treatment for breast cancer. Changes in the level of quality of life due to the determination of oncological diagnosis and subsequent treatment of a particular disease (according to the authors) are greatly affected by all aspects of quality of life of women, such as: social roles, functions, mental status, economic status, experienced emotions, social relationships of individuals. The process-model deals with the resultant action of individual areas and examines the quality of life experienced by the client after completion of oncological treatment. However, the relationship between life satisfaction and meaningfulness is also important from a different perspective. Studies have confirmed that they interact positively with each other [15]. Methods of measuring the quality of life in nursing are of great benefit for nursing practice. According to the survey, we found that nurses only know some methods to measure quality of life. Measurement of the quality of life in nursing has been influenced by the psychological approach (presented in the SWB construct) and the application of the medical approach (concept of HRQoL). SWB is an original psychological concept applied in the context of psychological research into quality of life. SWB is used in psychology to evaluate the quality of life as a whole. As part of the approach of SWB as well as the approach to quality of life, we encounter ambiguities and differing opinions. Generally, it is expressed mostly to describe, in relation to other related concepts. In anglosaxon literature, the most common terms such as satisfaction, happiness, well-being and so on in relation to the quality of life also include the concept of subjective well-being (well-being) and psychological well-being (psychological wellbeing) [12]. The selected model can be described as psychological, but some are based on the medical, sociological, and economic environment and have potential uses including in psychological research [16]. Other authors define subjective well-being as the evaluation of a person's life through cognitive and emotional reactions. They indicate what people think about their life, while maintaining their judgment and specific aspects of their life, such as work, marriage, etc. [17]. Such an evaluation of life describes the term subjective well-being, which includes several separate components: life satisfaction, satisfaction with key areas of life (e. g. satisfaction at work or in marriage), positive affect (experiencing pleasant emotions and moods), low negative affect [10]. The origin of subjective well-being at the psychological level is determined not only by the origin of the author and the sphere of the used constructs. Subjective well-being is assessed by a person by connecting the cognitive and affective levels to respond to events in the person's life.
CONCLUSIONS
Cummins [18] clarifies the stability of evaluation of the positive pole across different life situations. Psychology is ascribing interest to the subjective assessment of a person's life and “handling” of “soft” data that has its roots in introspection. The nature of this data can be illustrated by comparing the “objective, hard” data, which is used in other scientific disciplines [19]. Evaluation of quality of life depends on the level of education, cognitive intelligence and other factors: somatic, psychological, social, spiritual.


No Files Found




Internationally Accepted
Share Your Publication :