
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Wanyera Francis J* and Chombo Sammie Wale**
Corresponding Author: Wanyera Francis J, East African University, Kigali, Rwanda, **Chombo Sammie Wale, University of Tourism, Technology and Business Studies, Rwanda.
Received: October 10, 2024 ; Revised: February 04, 2025 ; Accepted: February 07, 2025 ; Available Online: February 17, 2025
Citation: Francis JW & Wale CS. (2025) Conservation and Sustainable use of Medicinal Plants in Mbale District: A case of Bukiende sub-county, Mbale District, Eastern Uganda. J Pharm Sci Drug Discov, 4(1): 1-14.
Copyrights: ©2025 Francis JW & Wale CS. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
Medicinal plants have been and still continue to play a crucial role in the world in terms of healthcare services especially in developing countries. The use of medicinal plants is critical for healthcare in rural Bukiende sub-county where significant portion of the population relies heavily on medicinal plant for primary healthcare. However, the rapid loss of flora due to overharvesting, habitat destruction and climate change poses a severe threat to these valuable resources. The sub-county of Bukiende is one of the biggest counties in Mbale District with population density estimated to be 435 individuals per square. Also, the problem was that the nearest health center for the population in this area of Bukiende is estimated to be far to access with an average distance of 45-57 kilometers away and thus seeking medicinal plants as alternative. It implied that the local community were unable to access health centers and resorted to traditional medicine as alternative. The general objective was to investigate the factors influencing conservation and Sustainable use of medicinal plants in Bukiende subcounty. The literature reviewed included the concepts, theories and studies that were guided by specific objectives. The methodology was descriptive and consisted of both qualitative and quantitative approaches. The primary and secondary data was utilized in this study. The target population of study was 213 households from three villages and a sample of 62 households as representative sample. The sampling techniques used were purposive and random sampling. The presentation of the findings was by use of figures, tables and essay form. The data collection tools included the group discussions, questionnaires, interviews and observation. Analysis of data was done by two methods that included; Informant Consensus Factor and Relative Frequency of Citation. The findings indicated that the key plant parts used included the leaves 29% and roots 22%. The key preparation method was cooking 55% and main administration method was oral 90%. Whereas the key factors that threatened the existence of the medicinal plants were; overharvesting 19%, and settlements 24%. Lastly, the key plant species identified to be of higher use value amongst the local community were Sapium ellypticum, Passiflora incarnata, Habiscus sabdariffa, Catharanthus roseus, persea americana. The suggested strategies comprised of creating awareness, involving local community and creation of cooperatives.
Keywords: Medicinal, Plants, Conservation, Sustainable use, Healthcare
INTRODUCTION
Medicinal plants have been and still continue to play a crucial role in the world in terms of health care services especially in developing countries [1,2]. Traditional medicine is the key source to treat humans and it is estimated that 80% of the population in developing countries depends on traditional medicine especially herbal medicine for primary health care [3,4]. The use of medicinal plants is preferred due to the fact that it is cheaper and easily accessible than the modern public health services [5,6] while in Africa, more than 80% of the population depends on traditional medicine for their health care needs. Further, Africa many places don’t have hospitals and even where they are existing, they are far from population [1,3,7-9] highlighted that in most cases in developing countries the local community walk on average 50 kms to access the modern health care services [10]. Many diseases such as malaria, tuberculosis, hepatitis, and typhoid fever have all along been treated by medicinal plants in both developed and developing countries [7,11,12].
Additionally, Tefera [11]; Ageh, and Lall [13] & Adom [14] emphasized that traditional medicines play a crucial role and at times it’s the only source of therapeutics for over 80% of the population in world. Another example highlighted is the estimated 500 m people in South Asian nations that are reported to indulge in health security from plants [3,15,16]. As a result, it is recommended by the World Health Organization that medicinal plant use should be adopted into the mainstream health system [6,9,17]. Due to scientific evidence supporting the efficacy of herbal medicine, efforts to improve and strengthen herbal medicine use is on a large scale. Studies also have revealed the significance of medicinal plants in the treatment of diabetes [10,18] and hypertension. Zhong, and Ma (2019), pointed out crucial need for medicinal plants in human health and well-being for decades. Besides, many different cultural groups in the world have been treating a number of ailments and illnesses by use of traditional medicine [3,13,19]. This is as a result of therapeutic properties of medicinal plants lie in their rich chemical composition that usually consists of bioactive elements with potential pharmacological capabilities [3,20,21].
Nevertheless, the increasing demand for medicinal plants influenced by factors that include population pressure, urbanization and increased interest in cheaper medicine, has exerted pressure on their sustainability [21]. Furthermore, factors such as habitat degradation, overharvesting, climate change and unsustainable harvesting activities [6,18]. Additionally, climatic variability is observed to affect plant phenology, alter habitats, floral distribution, change individual species population and interrupt harvesting periods of some medicinal plant species [19,22]. The decline of traditional- based conservation measures have been linked to ever changing societal dynamics as a result of religious influence, migrations, education and modernization [13,23]. That aside, it has also been discovered that absence of robust and supporting scientific knowledge, rising poverty, ignorance, unsustainable land practices, unemployment, and lack of unawareness of the value of these plants has been a great threat to conservation of these plants [6,24]. Additionally, pollination inadequacies, lack of sufficient potential seed dispersers and less productive plant distribution [3,22,25].
However, majority parts of the developing countries have less capacity to effectively assess the conservation status of medicinal plants and thus lack informed guidance on the prioritization of actual species for conservation and protection [7,23]. Without affecting the extraction and use of the medicinal plant species, sustainable harvesting is one reliable means to ensure that growing demand matches to considerable extent the supplies [12,26]. Sustainable harvest was noted as the most important conservation strategy particularly for wild harvested medicinal plants species [17,27]. However, major hurdles for a sustainable wild collection include ambiguous land use rights, ignorance on appropriate harvest practices, poverty, absence of relevant laws and policies, and weak traditional controls [11,25].
Generally, majority of the traditional medicines are gathered from the wild and the common reported threats include; overharvesting, unsustainable exploitation of medicinal plants for other purposes [6,22]. Other influences may include; unmonitored and unregulated trade, habitat and biodiversity loss, agricultural expansion and intensification. Additionally, human encroachment, irresponsible mining activities, uncontrolled urbanization, inadequate data on threatened medicinal plants and secretive nature of the traditional medicine practice [20,23,27]. Further, unfair competition from imported traditional medicines, convert bioprospecting and biopiracy, overgrazing and excessive browsing, population pressure, detrimental exotic and invasive plants, indiscriminate forest fires and adverse climate change [15,17,25]. Studies also indicate that majority traditional healers maintain secrecy for posterity and hence find it difficult to disclose or even patent the obscure components of traditional medicine as they directly affect their livelihoods [17,28,29]. In that regard, revealing of esoteric elements of traditional medicines comes with financial compensation, patenting or intellectual property rights, therefore secrecy carries out the role of patents [14,30].
The use of traditional complementary medicine in Uganda, particularly from plants has increased tremendously over the past two decades due to failure of some of the modern medicine [5,25]. However, the reliance on traditional complimentary medicine is threatening the loss of biodiversity of plant species, including medicinal trees, following unsustainable harvesting of tree parts [31,32]. In Tanzania and Uganda as many developing countries, medicinal plants are commonly used to treat various human diseases such as gastrointestinal disorders, malaria, stomach-aches, wounds, muscular pain, diarrhea, spiritual problems, psychiatric problems and other human diseases in both rural and urban communities [5,33,34]. Frequently used parts of medicinal plants include the roots, barks, leaves and flowers [7]. Furthermore, the emergence of new difficult to cure diseases such as malaria, strokes, diabetes, typhoid, cancer and heart diseases continue to exert pressure on the use of traditional plants [32]. Also, people in rural areas prefer to use medicinal plants due to high costs of modern medicines, including the high transport costs from the rural areas to urban medical centers [6]. While some believe that herbal medicine is more effective for certain diseases than conventional medicine [7].
On the contrary, the increasing demand for medicinal plants has been met by an indiscriminate harvesting of wild flora, including those found in forests. As a result, many plant species have become extinct and some are critically endangered [25,35]. As pointed out by Oryem [8]; Gumisiriza [28] many medicinal plant species or their populations are threatened by unsustainable intensities of use and patterns of harvesting. The collection of medicinal plants is unsustainable since it is not guided by laws of conservation in many communities [6,36]. Collection practices include uprooting, debarking or cutting fresh leaves from the plants [28,33].
Further, in Uganda, for example the frequency of herbal medicine use was estimated to be 60% [7]. The consumption is generally higher in rural areas, partly due to limited access to medicinal facilities, inadequacy and high cost of medicinal supplies. This accelerated by shortage and low motivation of medical practitioners, and wide acceptance of traditional medicines as having minimal side effects compared to conventional medicine [7,8]. In addition, medicinal plants in Uganda are collected from the wild using destructive harvesting techniques such as uprooting, debarking and cutting roots that threatens plant survival [1,32]. Nonetheless, wrong harvesting and consumption of herbal medicine is partly influenced by the increasing proliferation of unregulated herbal medicine business in urban centers. In the recent past Uganda has been listed among the countries that are facing the great risk of future extinction of medicinal plants [27,36]. Unfortunately, this coincides with Uganda’s up scaling of use of medicinal plants and its prospective integration into the main health care system. This is also supported by the Indigenous and Complementary Bill 2015 [31].
The eastern part of Uganda where the study was carried out is one of the poorest regions in Uganda with scanty health centers forcing majority of its people to rely on traditional medicine for the primary health care. In addition, the region has a characteristic topography and soil chemistry with mountainous areas in the Elgon region that extend to grasslands in Teso and Busoga regions which gives a unique rich vegetation that is used in traditional medicine. The rich flora in the region attracts traditional medicine practitioners from different parts of the country to harvest from it for the preparation of herbal remedies [37,38]. Due to these factors, Mbale district represents a promising region for investigating the use of plants in the management of variety of diseases such as malaria, hypertension and diabetes mellitus. Ethnobotanical studies play crucial role in documenting and preserving traditional knowledge about the use of medicinal plants, providing valuable insights into therapeutic properties, safety profiles and crucial significance.
The Elgon sub-region is one of the areas in Uganda that was blessed with assortment of medicinal plant species and the possibility that some have chronic illness such as cancer treatment benefits cannot be ruled out [39] Accurate documentation of traditional knowledge has always been critical for preservation and has served as a foundation for plant- based medication development [38]. However, the medicinal species have dwindled over time and yet indigenous knowledge of the plants used to treat sicknesses such cancer has not been extensively documented, despite the growing assumption of their use in this region [40]. Therefore, an ethnobotanical survey was conducted in the Elgon sub-region with the aim of identifying plant species used in the management of cancer.
Kudamba [40] carried out a study in Mbale district region and argued that the use of medicinal plant species varies from one part of the district to another as a result of differences in vegetation cover and cultural diversity. Majority of the population use variety of medicinal plants such as moringa oleifera, lam, Vernonia amyadalina, Dell, Warburgidia ugandenesis, Sprague, carica papaya. l, Annona muricate and biens Pilosa, to mention but a few were mainly reported to be used in the treatment of several diseases including cancer in the mount Elgon region, there is however, little accessible information is available about medicinal treatments of several illnesses that the local community suffer from in Mbale district.
Nankinga and Muwanga-Zake [41] emphasized that the conservation and sustainable use of medicinal plants in Bukiende sub-county situated in Mbale District located in Eastern Uganda is a pressing issue that stems from various interrelated factors. The district is rich in biodiversity, particularly in terms of flora, which includes numerous species of medicinal plants traditionally used by local community for healthcare. However, this wealth is increasingly threatened by several challenges that include; first of all, overexploitation because of the demand for medicinal plants which has surged due to both local and national markets. This overharvesting often occurs without regard for the sustainability of the species being harvested, leading to population declines [42]. Then the problem of habitat destruction as a result of agricultural expansion, urbanization, and deforestation which have significantly altered the natural habitats where this flora grows. As forests are cleared for farming or settlements, the ecosystems that support medicinal plant species are disrupted. In the same context, extensive lack of awareness problem among the local community about medicinal plants is crucial. In this case many of the local community may not fully understand the importance of sustainable and conserving their medicinal plant resources or the ecological roles these plants play. Additionally, the challenge of unpredictable climate change manifested in variation in climate patterns can affect the growth of conditions of many medicinal plants, potentially altering their availability and efficacy. The problem, is accelerated by rampant policy gaps that result from insufficient policies or enforcement mechanisms in place to protect these valuable resources from overexploitation and degradation [41].
This study was carried out in Bukiende sub-county because of knowledge gap for instance the sub-county has got one of the fastest growing population of 3.3% according to the population and housing census 2014 report. Further it has got limited medical facilities that creates high pressure for the populace to seek herbal medicine from medicinal plants as an alternative but there not any study yet. This study was also carried out in Bukiende sub-county due to the existing research gap about traditional medicinal plants in the district. This was evidenced by other studies carried out in other districts such as Tugume and Nyakoojo [7] Rukungiri District; Rahimi [10] in Butaleja District; Nuwaha and Musinguzi, (2019) in Mukono District. The study was guided by the following objectives; i) to determine the plant parts used for medicinal purpose ii) to ascertain the different core plant species that were used for medicinal treatment purposes iii) to investigate the threats to the conservation of the medicinal plants and strategies used to mitigate threats.
METHODOLOGY
Under this section, the study discusses the demographics, methods used, research design, approaches used, area of study, population od study, sample, sample size and technics used, data collection tools and data presentation.
Demographics
Demographically the population of majorly composed of the ethnic group of people called the bagisu. These are mainly rural community that practices subsistence farming as their main economic activity with majority living in abject poverty and have difficulties and limited access to the better medical facilities.
Area of study
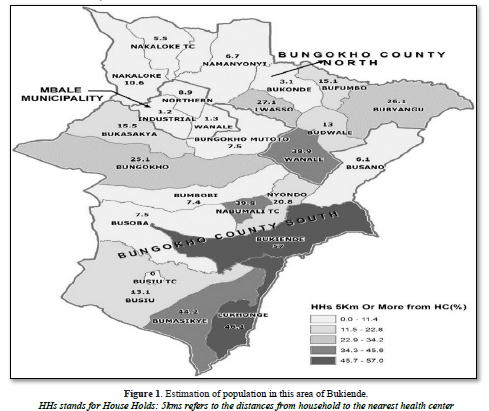
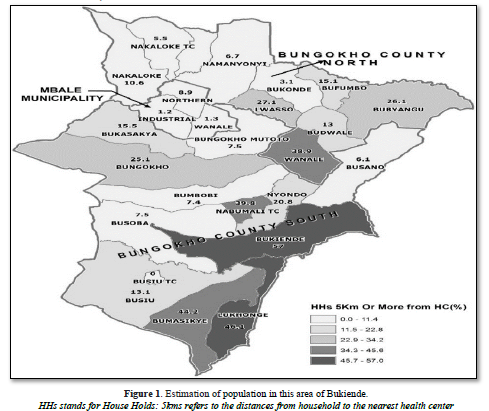
Mable district is bordered by Sironko District to the North, Bududa district to the Northeast, Manafwa District to the southeasy, Tororo District to the south, Butaleja District to the southwest and Budaka District to the west. The district is also bordered by Pallisa District and Kumi District to the northwest of Mbale District. Mbale, the largest town in the district and the location of the district headquarters, is located approximately 245 kilometers by road northeast of Kampala, the capital city of Uganda. The coordinates of the district are: 0057N, 34 20E. The District covers an area of 518,8 km2. The sub-county of Bukiende is bordered by Manafwa district and is one of the biggest counties in Mbale District. It covers an area of 40,09km2 with approximately a population of 262000 people with 3275 households. Its population density is estimated to be 430 individuals per square kilometer and annual population change of 3,3%. The gender in the sub-county is estimated to be 52.3% females and 47.7% males. The nearest health center for the population in this area of Bukiende is estimated to be on average 45-57 kilometers as indicated dark green color in Figure 1 below.
Field survey and data collection
The field guided surveys were conducted five times in two months from start of December to end of January 2023. The survey sites included three villages namely Bumaliro village, shibanga village and bumakika village by use of oral interviews, interview schedule, focus groups and participatory observation. A target population of 213 household of herbalists, elders and key informants from the three villages where a sample of 62 households were used. In the area participants from 62 households were interviewed including household leaders, key informants who consisted of renown traditional medicinal practitioners and elders. This was under the guidance of local council leaders and elders in the study area. Informed consent was obtained verbally from all participants prior to the study (International Society of Ethnobiology, 2006). The questionnaires were pre-tested for validity purposes to ensure collection of accurate data from the respondents.
Throughout the field survey, the informants were invited to list the medicinal plants that are still in use and this was in lugisu or luganda languages and translated to English. The interview was made up of two sections and the first part consisted of the informants (gender, age, education, occupation and location). The second section consisted of all medicinal plants including the locality of the reported medicinal plants, names, use-parts, processing methods, application methods, medicinal effects, conservation strategies and challenges. The data was collected, recorded and quantitatively analyzed using different indices. The nomenclature of all vascular plants follows the plants of the world online (https:/powo.science.kew.org) and the voucher specimens were deposited at the herbarium of Makerere University.
Data analysis and quantitative indices
The collected data were recorded and analyzed using Microsoft Excel 2018 for drawing figures in form of graphs and images. the categories suggested for diseases were classified according to International Classification of Primary Care (ICPC) (https;/www.who.int/classifications/icd/en/) system for intercultural comparisons, with minor modifications.
Relative Frequency of Citation: RFC= FC/N
The index showed the local importance of medicinal species by frequency of citation (FC) [43,44]. Relative frequency citation RFC= Fc/N where F is the number of informants that mentioned the use of the species and N is the total number of informants [45,46]. The frequency of citation divided by all the number of all informants participating in the survey (N). The higher the RFC, the more important the medicinal plant in in the area [43].
Informant Consensus Factor; ICF= Nur-Nt/Nur-1
Informant Consensus Factor analyzes the degree of difference in the type of medicinal plants used by different individuals to treat a certain type of disease. It can also reflect the importance of certain plants in the treatment of a certain type of disease in a specific cultural group. In the formula, Nur is the number of plant species recorded in the category and Nt is the total number of plant species recorded in the category. ICF values range from 0 to 1 and values close to 1 indicate that relatively few taxa are used by a large number of healers, or there is a clear standard for use of a specific plant species in the community. A low value close to 0 indicates that the informant does not agree with the use of the plant species in the above treatment categories [44].
RESULTS
Demographic characteristics of the respondents
The results indicated that respondents consisted of 62 informants from three villages who were interviewed. These comprised of 28 females (45%) and 34 males (55%). The results indicated that informants’ age ranged from 30 to 70 years and the majority 40% were in age range of 60 and 70 years while 20% were in age range 30 to 40 years, those in age range 40 to 50 were 25% and 50 to 60 years were also 25% respectively. The key informants belong to the Bagisu community from Bukiende sub-county and their education level was low with majority of respondents 42% were illiterates, 35 % were lower primary dropouts and 23% were lower secondary dropouts. The findings also revealed that the majority 90% of the informants were agriculturists ,10% were traders while 77% of the respondents had primary level education or illiterate with no education. These findings revealed that majority depended on medicinal plants for treatment of illnesses since had no employment and reliable income to afford better medication.
Diversity of medicinal plants
The results indicated that the Bagisu used a diverse number of medicinal plants. The 62 informants highlighted a total of 25 key vascular plant species used by the local community in Bukiende sub-county for medicinal purposes. These medicinal plants were majorly angiosperms and gymnosperms. These plants fall under angiosperms, and gymnosperms tracheophytes (kingdom plantae) basing on the two kingdoms system classification and the botanical scientific names. While the ethno-botanical data included; the medicinal parts, medicinal effect, mode of preparation and administration.
Used parts of medicinal plants
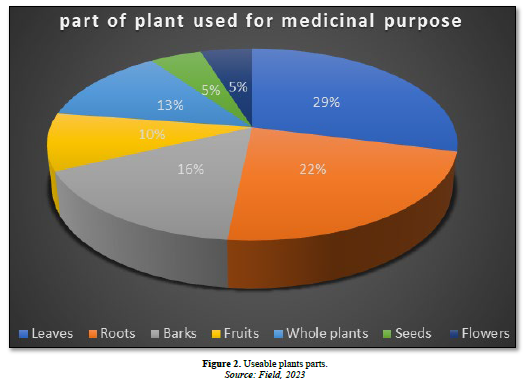
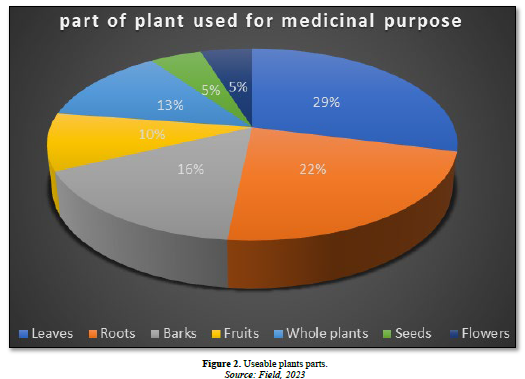
Results in Figure 2 revealed that the most frequently used parts were the leaves, roots, barks, whole plant, fruits and seeds. The findings in Figure 2 indicated that the local community (Bagisu) in Bukiende sub-county used the medicinal plants majorly their parts for several ailments. The different plant parts used for medicinal purposes are indicated in Figure 2 below. Results indicated that majority of the respondents totaling to29% agreed that leaves were the most used plant part for medicinal treatment purposes. For example, Aleovera spp, muringa olifera, bidens Pilosa, guava leaves, lemon grass and eucalyptus leaves were mentioned as the most used leaves for treatment of ailment. Additionally, results also indicated that plant roots were among the highly harvested plant parts that were used for medicinal purposes with 23% of the respondents who agreed. The participants pointed out for example Uncaria tormentosa, Zingber officinale and kigeria Africana among others were frequently used. Some respondents argued that apart from the leaves and roots, there were diseases that were treated by use of plant barks and 16% of the respondents concurred. Key main examples of the plant barks used were Catharanthus roseus and Eucalyptus globulus. Interestingly the results revealed that some treatments involved using the whole plant. In this case 13% of the respondents agreed that some diseases required getting the whole plant in to use for treatment such as stomach upsets. In addition, the study found out that some illnesses were treated by use of plant fruits and 10% of the respondents agreed. For example, the respondents pointed out the Prunus spp, Citrus limon, Mormodica charintia and Psidium guajava were frequently used for the treatment of illnesses such as coughs and flue. Lastly, the results indicated that seeds and flowers were harvested for treatment of certain illnesses. The results indicated further that 5% of the respondents respectively agreed that the seeds and flowers played a vital role in treatment of the local community. For example, the Sapium ellypticum, Passiflora incarnata, Habiscus sabdariffa, Catharanthus roseus, persea americana, carica papaya and cucurbita pepo seeds are used for stomach illnesses though they were not extensively applied.
Modes of preparation and administration
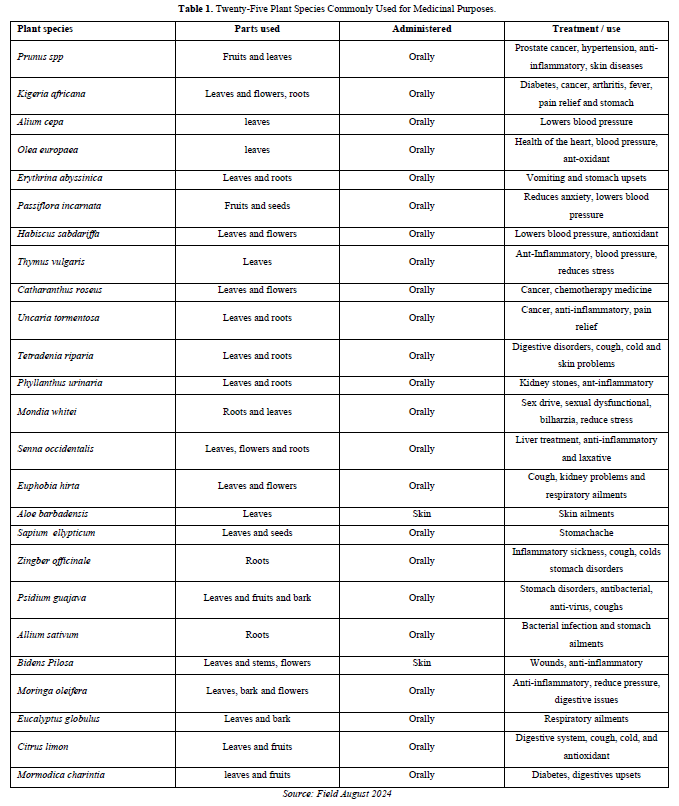
The findings in Table 1 revealed that the preparation and administration of these extracted medicines from the harvested plant parts was done in different ways depending on the part of the plant harvested. The participants however, highlighted the main extraction and administration methods commonly used. The study discovered that the majority of the respondents totaling 55% agreed that the most used mode of preparation was cooking particularly boiling the medicinal plant part harvested. They argued that boiling enabled the extraction of required medicinal elements to dissolve the water that can be used for the treatment of the illnesses. The commonly used administration for the medicine extracted through this process was oral administration. The results also indicated that de-connection was another key method commonly used and was agreed by 25% of the respondents. The de-connection method was involved filtering out the required useful medicine and it was also administered orally. The respondents agreed that this was commonly used to reduce the concentration of the extracted medicine not to be harmful to the sick. Results from the study also indicated that crushing was another frequently used method and 13 % of the respondents agreed. They emphasized that the crushing process was to ease digestion of the orally taken medicine but also for external administration especially the skin ailments. Lastly, grinding of the plant part into powder form specially from dried fruits, leaves and seeds. This was supported by 7% the respondents. The majority of the respondents concurred that powder medicine was primarily administered orally with minority who agreed it was applied externally for skin diseases.

Relative frequency of citation and informant consensus factor
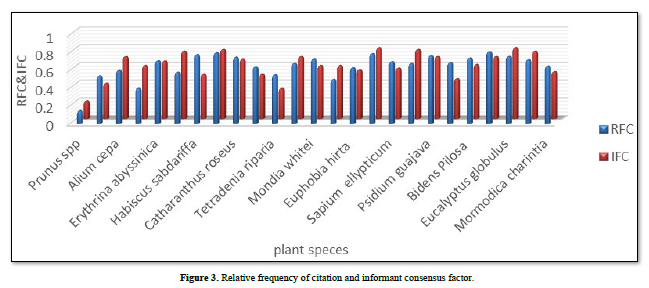
Findings in Figure 3 below indicated analyzed data about the frequency at which the particular medicinal plants were used and the consensus about plant use on particular illnesses. Under this study, 25 key frequently used plant species were analyzed as shown in Table 2 and the study used a formula RFC= Fc/N where F was the number of informants that mentioned the use of the species and N was the total number of informants and their values ranged between 0 to 1. Whereas Informant Consensus Factor (IFC) analyzed the degree of difference in the type of medicinal plants used by different individuals to treat a certain type of disease. Both RFC and ICF values ranged from 0 to 1, where 0 is lowest and 1 highest as indicated in Figure 3. The formula, Nur was the number of plant species recorded in the category and Nt is the total number of plant species recorded in the category. The results were analyzed and indicated that the majority of values of both RFC and IFC were above 0.5 which clearly indicated the frequently used plant species and plant parts. The IFC results revealed the frequency above 0.6 which also indicated that majority of the respondents expressed wealth of knowledge about the plant medicine used and the illnesses they treated. It was discovered that Prunus spp, Alium cepa, tetradenia riparia and Psidium guajava were some of the plant medicines with low information consensus factor but the rest were discovered to have a high factor However, some of these medicinal plants that had a low IFC indicated a high RFC and this displayed that the local community had high knowledge about the plants used for medicinal purposes and the illnesses they treated accordingly.
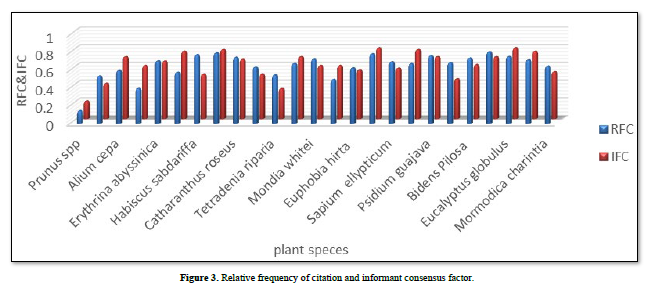
Figure 4 below indicates some of the medicinal plants with the names in local language and what they treat.
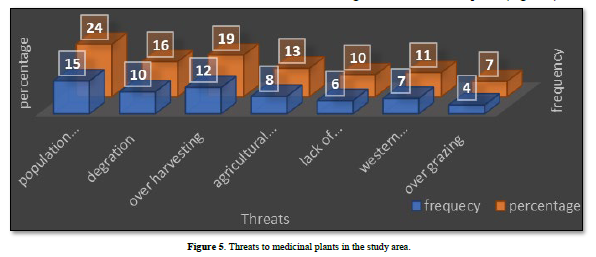
The study findings about the threats to the medicinal plants in Bukiende sub-county, majority of the respondents agreed that for the past two decades, the rapid population growth threatened the medicinal plants due to increased demand for land for settlement. In the same line of argument 24% of the respondents, expressed concern that population pressure had increased and led to rampant clearance of land to construct homes and hence destroyed the medicinal plants. Besides, results revealed that high numbers of respondents also expressed worry about overharvesting of the medicinal plants. The results indicated that 19% of the respondents emphasized that due to financial benefits attached to the medicinal plants, many people indulged in harvesting and selling for income. In addition, the problem is worsened by the lack of health centers in Bukiende subcounty where the local community travelled for more than 50 kilometers to get treatment as indicated in Figure 4 (map) in chapter three. Further, the findings showed that some respondents agreed that agricultural expansion was a big threat to medicinal plants. The results revealed that 13% concurred that as population increased, more land for cultivation was demanded and in the process of clearing land for agriculture, the medicinal plants were destroyed. Another threat voiced by the respondents was the threat of western medicine.

The findings found out that 11% of the respondents expressed fear about the modern medicine. They emphasized that western medicine had been taken to be more effective than the traditional ones and so the local community sought for them and ignored the original medicinal plants for treatment. The study findings also revealed that one of the threats in the area was lack of knowledge among some of the local community about the importance of the medicinal plants in the treatment of certain ailments. In the same line 10% of the respondents expressed ignorance when asked about the medicinal use of certain medicinal plants. The respondents said they thought such plants ended with the great grandfathers and no such a thing still works. Lastly, the results indicated that most of the plants were threatened by the domestic animals especially over grazing. This was attributed to the shortage of land and so many animals utilized the few plots of land which intensified grazing, hence degradation of medicinal plants (Figure 5).
Strategies used to mitigate threats to conservation of medicinal plants
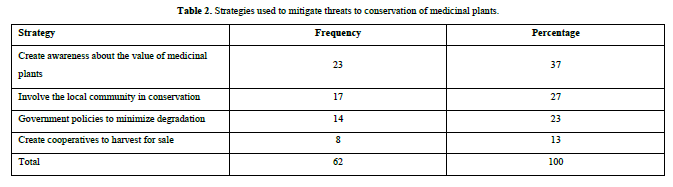
The study after discovering the threats to the medicinal plants, the following suggested strategies were pointed out to minimize the rate at which the medicinal plants were threatened. The results revealed that 37% of the respondents agreed that creating awareness about the value of the medicinal plants was the best strategy that could be applied. This was suggested because many of the respondents concurred that majority of the community especially the youth were not aware of the importance. Findings also indicated that one of the suggested strategies was the involvement of the local community in conservation of these medicinal plants. The local community expressed interest in playing a role to conserve the medicinal plants because they treated everyone regardless of the age. The study also suggested that the government should formulate and implement the policies that protect the valuable medicinal plants such that they are sustainably harvested. The strategy was suggested by 23% of the total respondents and it indicated how important the role of government was in such natural resources. Lastly, the study revealed another strategy suggested by 13% of the respondents and they argued that these medicinal plants could be conserved through formation of local community cooperatives to monitor how they harvested and used as well as income earned from them (Table 2).

DISCUSSION
Plants played a crucial medicinal role and results revealed that the most frequently used parts were the leaves, roots, barks, whole plant, fruits and seeds. Majority of the respondents agreed that leaves were the most used plant part for medicine. For example, Aloe barbadensis, moringa aleifera, bidens Pilosa, Psidium guajava, Cymbopogon citratus and eucalyptus spp among others. While results also indicated that plant roots were among the highly harvested plant parts that were used for medicinal purposes for example Uncaria tormentosa, Zingber officinale and kigeria Africana among others the results concur with Tugume and Nyakoojo [7], Tefera [11] & Abera [12] who agreed that many diseases such as malaria, tuberculosis, hepatitis, and typhoid fever have all along been treated by medicinal plants in both developed and developing countries.
Additionally, some respondents agreed that instead of leaves and roots, other diseases were treated by use of barks and the main examples of the plant barks used were Catharanthus roseus and Eucalyptus globulus. These findings agreed with Zhong, and Ma (2019), who pointed out crucial need for medicinal plants in human health and well-being for decades. As well, Cheung [3], Ageh and Lall [13] & Bennet [19] mentioned that many different cultural groups in the world have been treating a number of ailments and illnesses by use of traditional medicine. Interestingly the results revealed that some treatments involved using the whole plant. While, the study also found out that some illnesses were treated by use of plant fruits. For instance, Prunus spp, Citrus limon, Mormodica charintia and Psidium guajava among others. Lastly, seeds and flowers were also harvested for treatment of certain illnesses. The findings concurred with earlier researches that found out that different plant parts were harvested to treat different sicknesses. These included studies done in Uganda and Tanzania that discovered that medicinal plants were commonly used to treat various human diseases such as gastrointestinal disorders, malaria, stomach-aches, wounds, muscular pain, diarrhea, spiritual problems, psychiatric problems and other human diseases in both rural and urban communities. Frequently used parts of medicinal plants included the roots, barks, leaves and flowers. Also, in agreement with the findings were studies that highlighted that in most African traditional societies, herbal medicine was often prepared as crude extract of medicinal plant organs such as leaves, roots, flowers and barks.
The study indicated that the majority of the respondents agreed that the most used mode of preparation was cooking particularly boiling the medicinal plant part harvested. The commonly used administration for the medicine extracted through this process was oral administration. The results also indicated that de-conction was another key method commonly used and was agreed by 25% of the respondents. The respondents agreed that de-conction method was commonly used to reduce the concentration of the extracted medicine not to be harmful to the sick. Crushing was another frequently used method and they emphasized this process was to ease digestion of the orally taken medicine or eaten as food. However, for external administration it was applied on the skin ailments especially wounds. Lastly, grinding of the plant part into powder form specially from dried fruits, leaves and seed.
The study findings about the threats to the medicinal plants in Bukiende sub-county, majority of the respondents agreed that for the past two decades, the rapid population growth threatened the plants due to increased demand for land for settlement. Similarly, respondents, expressed concern that population pressure had led to clearance of land to construct homes and consequently destroyed the medicinal plants. Besides, results indicated that due to financial benefits attached to the medicinal plants, many people indulged in over harvesting and selling for income. In addition, the problem was worsened by the lack of health centers in Bukiende subcounty where the local community traveled for more than 50 kilometers to get treatment. Further, agricultural expansion was a big threat to medicinal plants. As population increased, more land for cultivation was demanded and in the process of clearing land for agriculture, the medicinal plants were destroyed. Western medicine had been taken to be more effective than the traditional ones and so the local community embraced them and ignored the original medicinal plants for treatment. Lack of knowledge among some of the local community about the importance of the medicinal plants in the treatment of certain ailments was another threat. Ignorance about medicinal plant use for the treatment of certain illnesses were a threat. Lastly, over grazing threated the plants especially the domestic animals. Previous studies agreed with the findings that the reliance on traditional complimentary medicine is threatening the loss of biodiversity of plant species, including medicinal trees, following unsustainable harvesting of tree parts. In addition, the findings concurred with earlier researchers such as Di Minin (2019) and Sharma and Kala (2022) that many medicinal plant species or their populations are threatened by unsustainable intensities of use and patterns of harvesting. According to Tesfahuneygn and Gebreegziabher (2019); Asmare (2018) medicinal plants were threatened through Collection practices that included uprooting, debarking or cutting fresh leaves from the plants.
The following suggested strategies were pointed out to minimize the rate at which the medicinal plants were threatened. Majority agreed that creating awareness about the value of the medicinal plants was the best strategy that could be applied. It was because majority of the community especially the youth were not aware of the importance of these plants. Another suggested strategy was the involvement of the local community in conservation of these medicinal plants. Further, the government should formulate and implement the policies that protect the valuable medicinal plants for sustainable harvesting. Another strategy suggested formation of local community cooperatives to monitor how they harvested and used these medicinal plants as well as income earned from them. The findings agreed with researchers on formulation of policies to protect the plants. Results agreed that the use of traditional complementary medicine, particularly from plants has increased tremendously over the past two decades due to failure of some of the modern medicine [25]. This is also supported by the Indigenous and Complementary Bill 2015 [31].
Analyzed data about the frequency at which the particular medicinal plants were used and the consensus about plant use on particular illnesses. The study sampled, 25 key frequently used plant species and used RFC= Fc/N, whereas, Informant Consensus Factor (IFC) analyzed the degree of difference in the type of medicinal plants used by different individuals to treat a certain type of disease. Both RFC and ICF values ranged from 0 to 1, where 0 is lowest and 1 highest as indicated in Figure 1. The formula, Nur was the number of plant species recorded in the category and Nt is the total number of plant species recorded in the category. The results were analyzed and indicated that the majority of values of both RFC and IFC were above 0.5 which clearly indicated the frequently used plant species and plant parts. The IFC results revealed the frequency above 0.6 which also indicated that majority of the respondents expressed wealth of knowledge about the plant medicine used and the illnesses they treated. It was discovered that Prunus spp, Alium cepa, tetradenia riparia and Psidium guajava were some of the plant medicines with low information consensus factor but the rest were discovered to have a high factor. However, some of these medicinal plants that had a low IFC indicated a high RFC and this displayed that the local community had high knowledge about the plants used for medicinal purposes and the illnesses they treated accordingly.
CONCLUSION
It was concluded that traditional medicinal plants played a crucial role in the lives of the Bagisu community in Bukiende sub-county for several decades and due to increased demand and financial benefits attached to the medicinal plants, there was rapid disappearance and rampant degradation of these plants. The Bagisu in Bukiende harvested different parts of the medicinal plants for treatment of different diseases. These harvested plant parts included the leaves, roots, bark, flowers, fruits and seeds. The most frequently harvested plant species were those that were deemed effective to particular ailments by the local community for instance Aloe barbadensis, moringa aleifera, bidens Pilosa, Psidium guajava among other twenty-five key species. Additionally, major threats to medicinal plants in Bukiende sub-county included mainly human activities such as population growth, agriculture expansion, overharvesting, lack of awareness and overgrazing. Lastly, to curb these threats the respondents suggested that strategies such as creating awareness, involving the local community in policy formulation, creating cooperatives for all-inclusive purposes and the government implementing strong policies to minimize extinction of the crucial medicinal plants to be employed [47,48].
RECOMMENDATIONS


No Files Found




Internationally Accepted
Share Your Publication :