
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Shōbo A*
Corresponding Author: Shōbo A, Associate Professor, Bunkyo Gakuin University, Faculty of Health Science Technology, Department of Physical Therapy, Saitama, Japan
Received: April 05, 2022 ; Revised: April 10, 2022 ; Accepted: April 23, 2022 ; Available Online: May 1, 2022
Citation: Shōbo A. (2022) Effects of Sitting Position on Volumes of Hemi thoraces of Healthy Men and a Patient Who Underwent Thoracotomy with a Midline Incision. J Ageing Rehab Res, 1(1): 1-4.
Copyrights: ©2022 Shōbo A. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
INTRODUCTION
In clinical practice physical therapists encounter patients with poor posture that may lead to changes taking place in the mechanics of thoracic excursion with accompanying abnormal breathing patterns. The thoracic cage principally consists of the thoracic vertebrae, ribs and sternum. If an incongruity, albeit a small one, occurs in this structure, its mechanics will be affected, resulting in a significant impact on respiratory function. Therefore, it was considered significant to clarify the relationship between changes in thoracic configuration and respiratory function.
During the assessment of patients with fatigue and dyspnoea, it was frequently observed that right-left asymmetry of respiratory muscle activity occurred. This asymmetrical movement included abnormal alignment of the thorax on a sagittal plane, changes in thoracic configuration in relation to the pelvis on a frontal plane and right-left discrepancy in chest expansion. Further, in a study carried out on thoracic configuration in relation to the alignment of the pelvis on a frontal plane right-left discrepancy in chest expansion was observed.
post-thoracotomy patients may acquire restrictive lung expansion due to poor posture. It is important to understand thoracic configuration and chest movement. Anomalous alignment of the thorax may be evident in patients with respiratory conditions and post-thoracotomy. This leads to asymmetrical displacement of the thorax against the pelvis with differences in expansion during breathing. The aim of this study was to compare the left and right thoracic contours at different loci on the thorax.
METHODS
Participants
The participants were one post-thoracotomy patient with a midline incision and 11 sedentary non-smoking healthy men with no history of respiratory or spinal condition. They had a mean (SD) age of 21.6 (1.6) years (range: 20-26), mean (SD) body mass of 59.8 (10.0) kg (range: 48-76), mean (SD) height of 169.7 (4.8) cm (range: 162-176) and a mean (SD) body mass index of 20.7 (2.7) kg/m2 (range: 17.30-24.53). The investigators explained to the participants the purpose and procedures of the study and obtained their written consent for participation.
Procedure
The participants were tested in two sitting positions. These were an upright sitting position with a pelvic tilt of zero degrees and a hunchbacked sitting position with a pelvic tilt of 20 degrees. For both positions the feet were flat on the floor and the hip and knee joints in 90° of flexion. The pelvic angle was defined as an angle created by intersecting imaginary lines formed by infrared reflective markers attached to the skin over the anterior and posterior superior iliac spines. This was in conjunction with an imaginary spatial horizontal line, which was determined by using a spirit level.
A total of 84 infrared reflective markers each with a diameter of 9.5 mm were placed at specific points on the skin over the anterior and posterior aspects of the trunk. Any changes in their movement recorded changes in thoracic volume. The precise positioning for both the anterior and posterior markers was determined from six midline markers placed vertically in line on six levels, these being the sternal notch, third rib, xiphoid process, eighth rib, tenth rib and umbilicum, all of which are commonly used as a guide for palpation of chest movement. In relation to the six midline markers on the trunk an additional 78 markers, in order of their proximity to them, were placed medially, centrally and laterally on the anterior and posterior aspects of the trunk. Specifically, three markers were placed on either side of a midline marker, totaling seven markers in all.
The distance between each marker was based on the participant’s physique and set at 15% of the distance between the left and right acromion processes. This procedure was repeated on the posterior aspect of the trunk at each of the corresponding six levels.
The anterior half was encompassed within the space of the upper thorax demarcated by the sternal notch and third rib, and the posterior half within the space of the lower thorax demarcated by the xiphoid process and tenth rib. Using a three-dimensional motion analyzer Vicon MX (Vicon, Inc.), the difference in volume within the upper and lower hemi thoraces was measured in the two sitting positions during quiet breathing and volitional deep breathing, each with five or more consecutive breaths. An average value of three consistent breaths was taken for the calculation. In accordance with previous studies [1-6], the changes in thoracic volume were calculated from the amount of change in the movement of the infrared reflective markers attached to the body surface. For recording of this movement, seven infrared cameras were used, and the data were stored on a personal computer with a sampling frequency of 100 Hz.
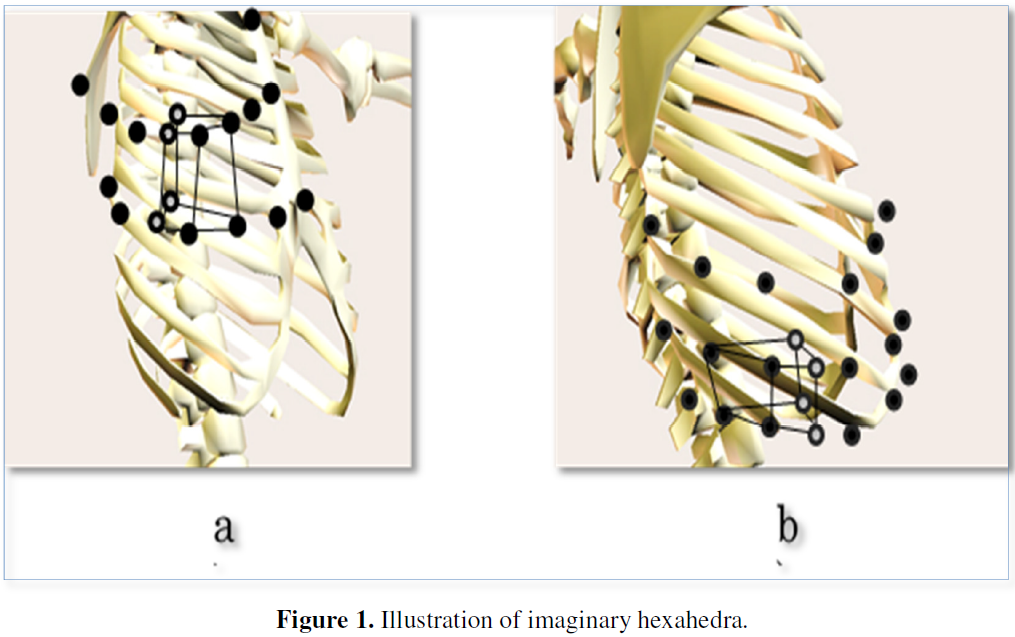
The thoracic volume was calculated in accordance with the method developed by Ferrigno and Carnevali [1] and Nakabo and Yamamoto [3]. Specifically, six imaginary hexahedra were visualized for the upper thorax with three for the right and three for the left using four markers for each on the anterior and posterior aspects of the thorax at the levels of the sternal notch and third rib (Figure 1a). Similarly, this was repeated for the lower thorax at the levels of the xiphoid process and tenth rib (Figure 1b). Further, each of these imaginary hexahedra was, then, divided into three imaginary triangular pyramids to calculate positional vectors using the data obtained from the position of each marker in accordance with the method employed by Ferrigno and Carnevali [1]. Finally, the volume for both the hexahedra and triangular pyramids was calculated, culminating in any change of thoracic volume on a whole.
To measure for any changes in the thoracic volume imaginary midpoints were established between the ventral and dorsal markers with the upper thorax encompassing the anterior space between the ventral markers and their midpoints. Similarly, the lower thorax encompassed the posterior space between the dorsal markers and midpoints. This measurement method was based on the model originally developed by Shōbo and Kakizaki [7] for analysis of thoracic movement (Figure 1). Thereby, the volume change in each hexahedron could be calculated. Accordingly, four thoracic volumes were measured: a) the upper right and left hemi thoraces’ volumes emanating from a midpoint on an imaginary line connecting from the sternal notch to the third rib; and b) the lower right and left hemi thoraces’ volumes emanating from a midpoint on an imaginary line connecting from the xiphoid process to the tenth rib. The Vicon Body Builder and MATLAB (MathWorks, Inc., Natick, U.S.A.) were used for calculation of the thoracic volumes.
For statistical analysis, the Wilcoxon rank-sum test was employed for comparison of the changes in volume of the bilateral hemi thoraces. The level of significance was set at p<0.05, and, for the data analysis, the Statistics Package for Social Sciences version 23.0 (SPSS Japan Inc, Tokyo, Japan) for Windows was employed. This study was approved by the Bunkyo University Medical Ethics Review Board (Approval No. 2016-0034).
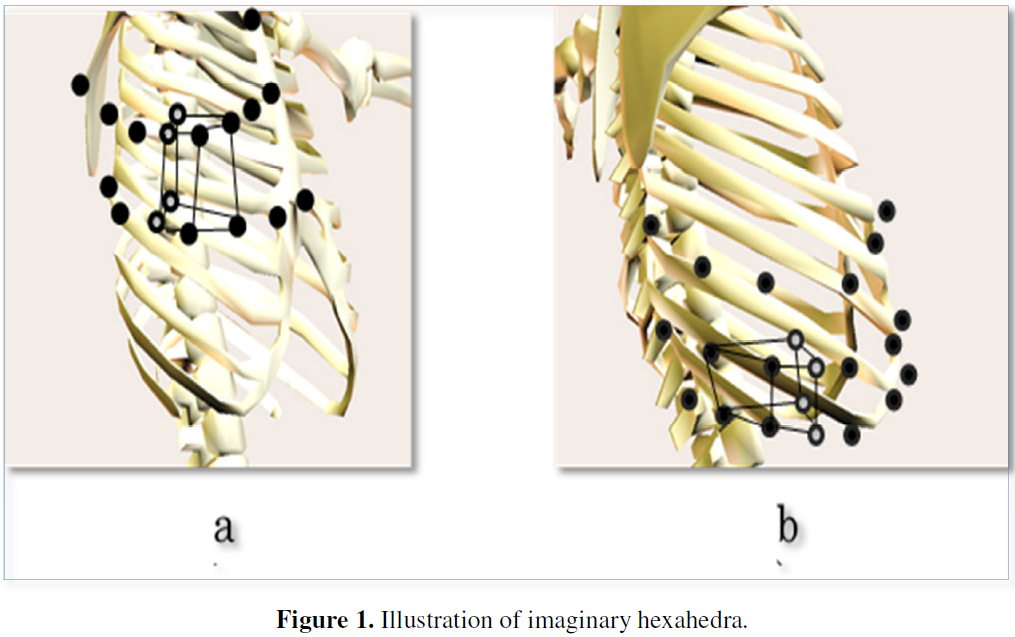
Dots indicate markers from which the hexahedra were constructed. Circles indicate imaginary midpoints.
RESULTS
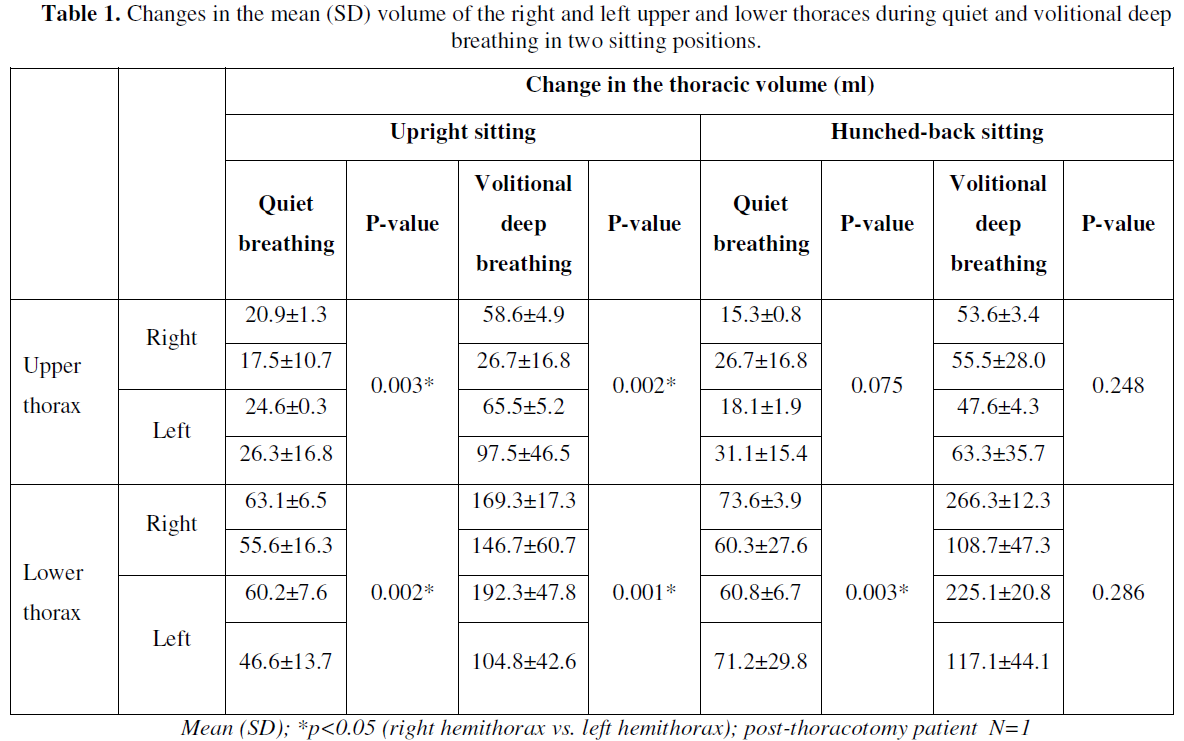
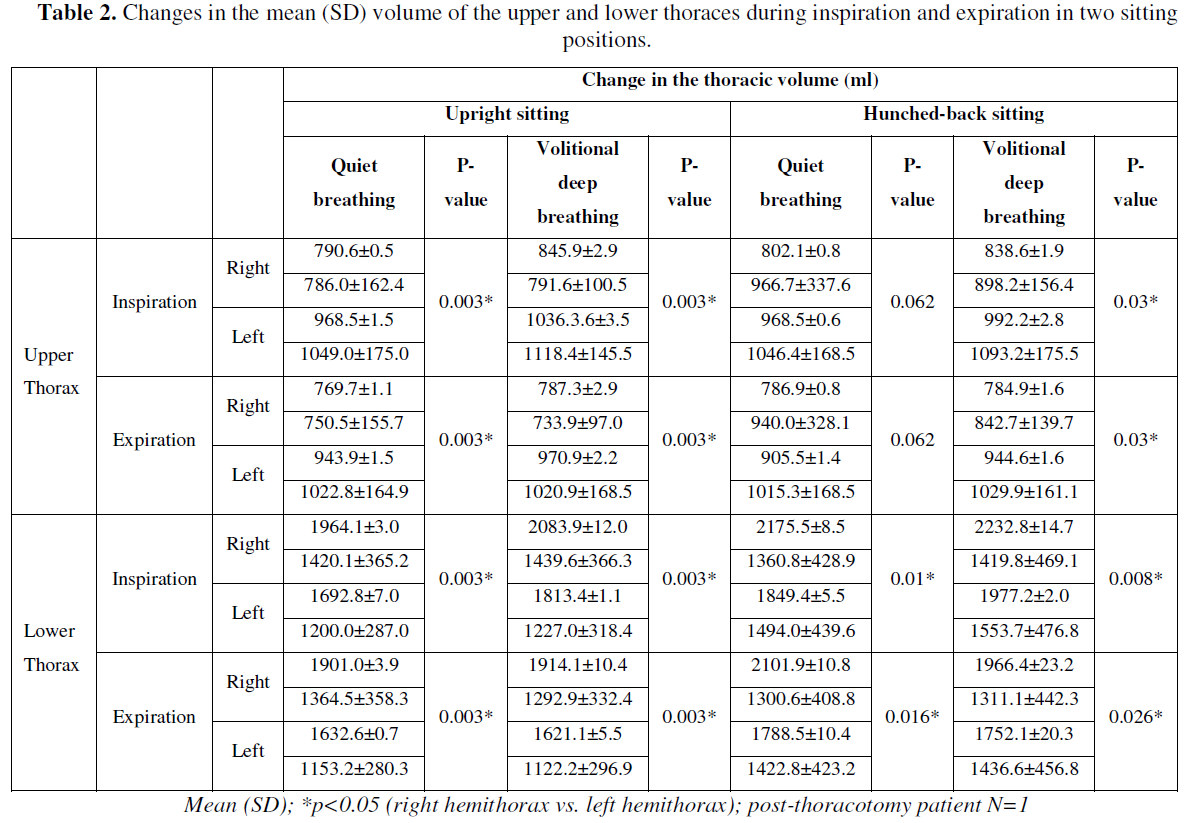
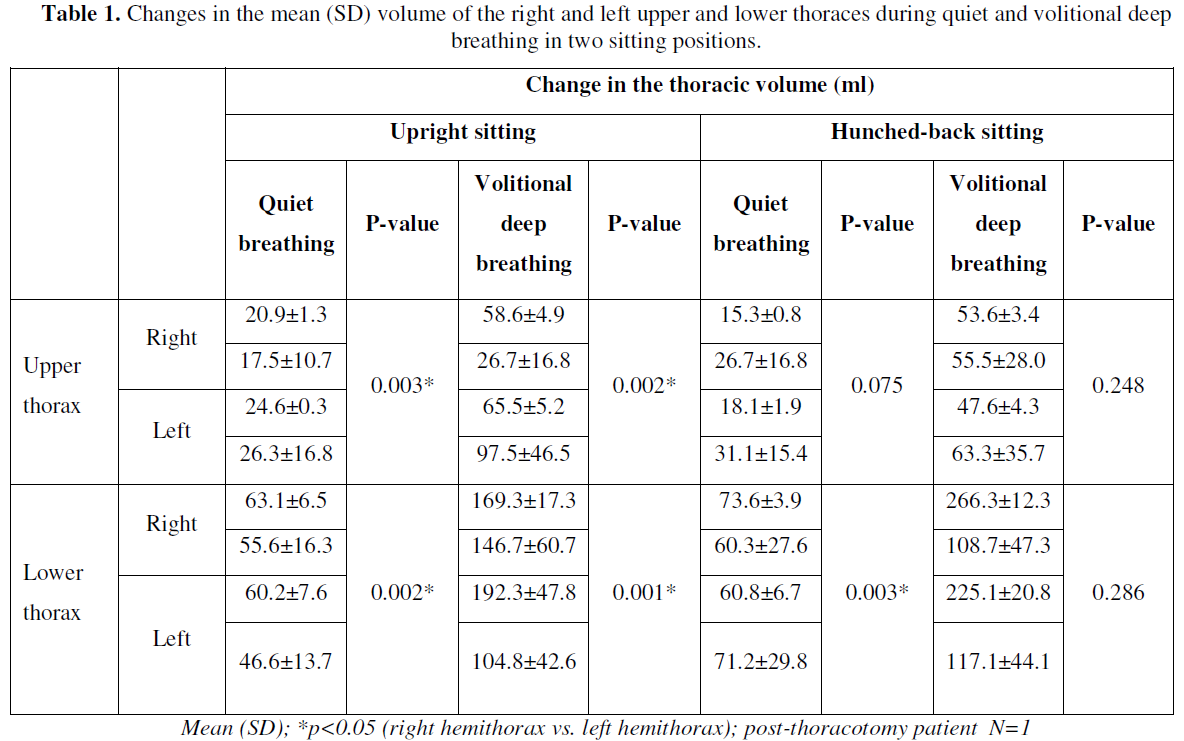
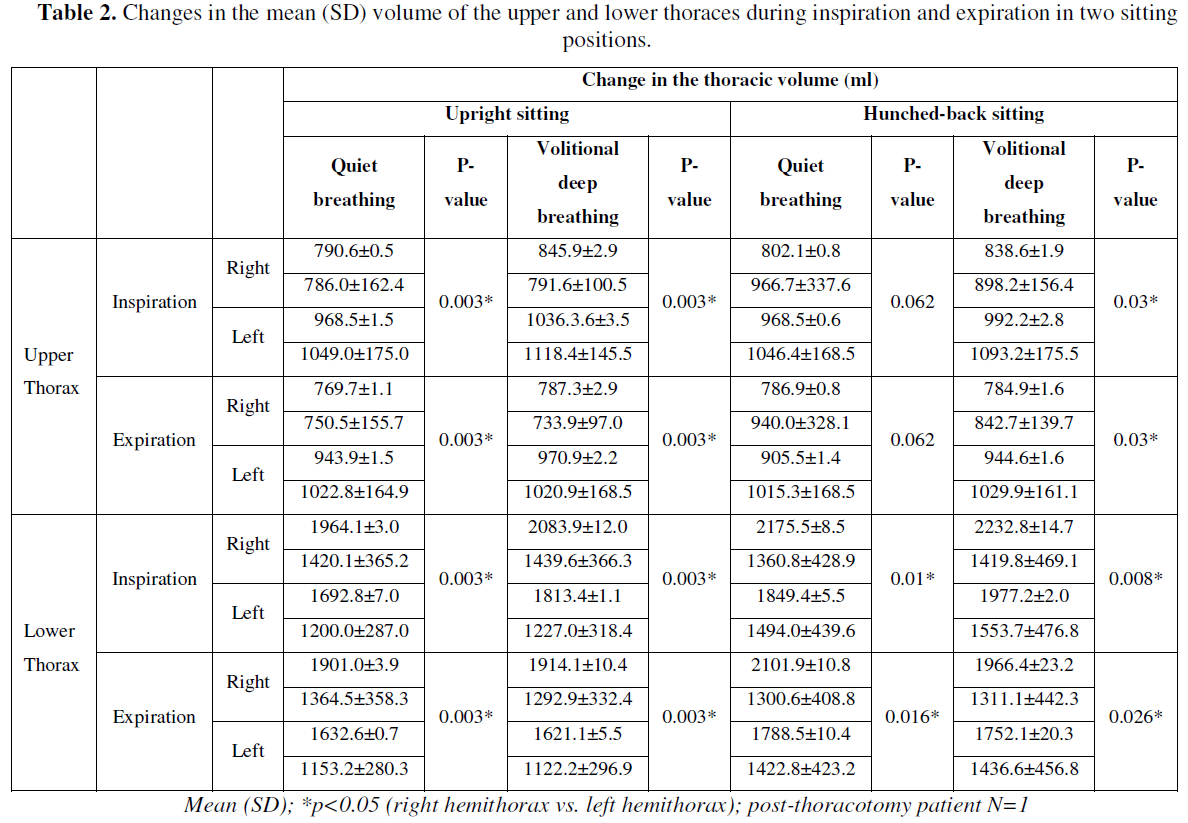
For all participants in stooped sitting for both breathing patterns, the left upper hemithorax showed significantly greater change in upper thoracic volume and significantly greater change in thoracic configuration on termination of inspiration and expiration. For the healthy men, the left lower hemithorax showed significantly greater change in thoracic configuration and lower thoracic volume on termination of inspiration and expiration. For the patient in the right lower hemithorax, there was a significantly greater change in thoracic configuration and lower thoracic volume on termination of inspiration and expiration for both breathing patterns (Tables 1 & 2).
DISCUSSION
In healthy men at upright sitting, the left upper thoracic configuration was larger than the right, and this was reversed for the lower thoracic configurations even during volitional deep breathing in hunchbacked sitting the upper ribs of the thorax rotate anteriorly with the costovertebral joints fixated anteriorly leading to posterior rotation of the ribs, consequently, limiting rib elevation [7]. However, for the patient in the right lower hemithorax, there was a significantly greater change in thoracic configuration and lower thoracic volume on termination of inspiration and expiration for both breathing patterns. In other words, there is not the difference of right and left by the lower thoracic volume change during volitional deep breathing at hunchbacked sitting in healthy men, but in the patients, the right low thoracic configuration was larger than the left [7]. In addition, in healthy men at hunchbacked sitting during volitional deep breathing, the left upper thoracic configuration was larger than the right, and the right low thoracic configuration was larger than the left in the patients. The difference is seen in the pattern corresponding to the posture change when I divide it into expiration and inspiration. As for this, a breathing pattern is fixed in the patients, and it is thought that it is in condition not to be able to raise the change of the breathing pattern depending on a posture change.
Therefore, it would be of interest in the future to further investigate and verify this factor.
CONCLUSION
In the patient with a median sternotomy, left thoracic deviation was apparent during quiet expiration during upright sitting and, also, in hunched-back sitting with no neutralization of the thoracic contour.
Limitations of this study were that activity of the erector spinae was not examined in this study. However, future studies are required to investigate the role of this muscle in relation to respiratory function in various postures, together with abdominal external oblique, serrates anterior and latissimus dorsi muscles. In addition, our study population was rather small.
REFERENCES
No Files Found




Internationally Accepted
Share Your Publication :