
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Mahnoor Bajwa, Umair Arif*, Khadija Sharif, Anam Maqbool, Komal Razzaq and Sana Aiman
Corresponding Author: Umair Arif, Lecturer at The University of Faisalabad, West Canal Road, The University of Faisalabad, Pakistan.
Received: April 16, 2021 ; Revised: April 19, 2022 ; Accepted: April 22, 2022 ; Available Online: May 1, 2022
Citation: Bajwa M, Arif U, Sharif K, Tariq U, Maqbool A, Razzaq K, et al. (2022) Effects of Modified Gait Pattern with Isometric Exercises on Range of Motion (Hip & Knee) Flexion in Knee Osteoarthritis Patient. J Ageing Rehab Res, 1(1): 1-8.
Copyrights: ©2022 Bajwa M, Arif U, Sharif K, Tariq U, Maqbool A, Razzaq K, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
Abstract
Objective: To identify the effects of modified gait pattern with isometric exercises on ROM (hip & knee) flexion in knee osteoarthritis patients.
Methodology: Quantitative comparative study was conducted. The subjects were knee osteoarthritis patients with grade 3 & 4 of Kellgren Lawrence scale who were at greater risk of falling due to osteoarthritis. The half of patients received modified gait pattern along with isometric exercises and other half received isometric exercises. Government setting was Allied Hospital, Faisalabad. Private setting was Irfan medical city, Faisalabad. Independent sample t-test was applied for comparison between groups. Repeated Measure ANOVA was used to check the effects within groups. Significance is checked at p-value less than 0.05.
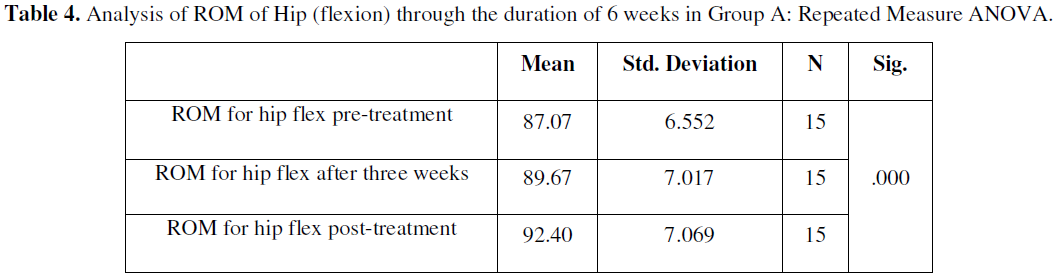
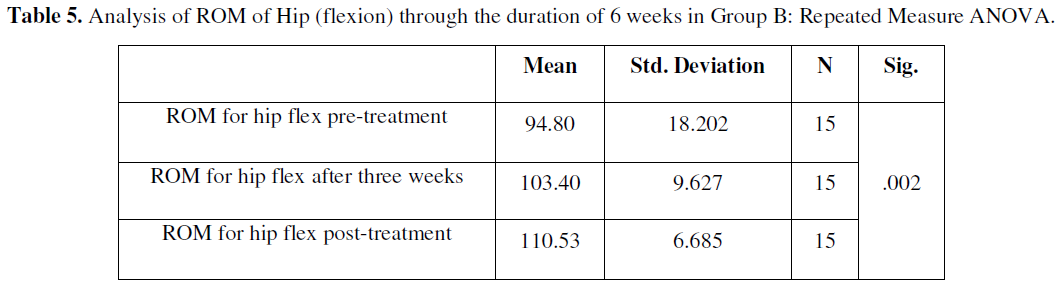
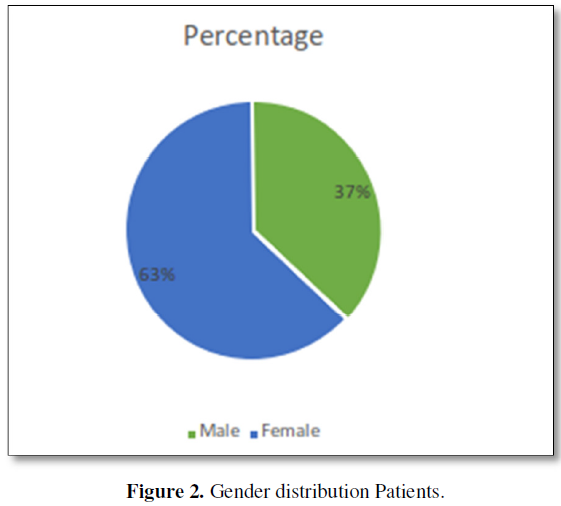
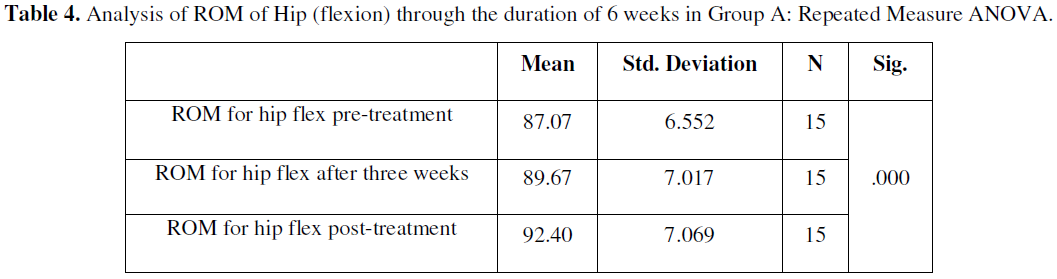
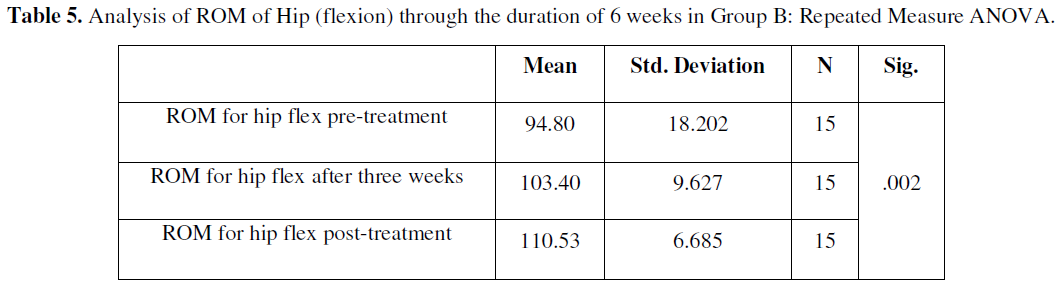
Results: Overall average ± S.D of age of patients were 55.89 ± 3.52. 63% (19) participants were from female category of gender while only 37% (11) male participants were enrolled into the study. the value of p is less than 0.05 which means it is statistically significant while the mean changes from 87.07±6.552 at baseline to 89.67±7.017 at 3rd week to 92.40±7.069 at the end of treatment of participants of group A. the value of p is less than 0.05 which means it is statistically significant while the mean changes from 94.80±18.202 at baseline to 103.40±9.627 at 3rd week to 110.53±6.685 at the end of treatment of participants of group B.
Conclusion: Modified gait pattern along with isometric exercises showed effectiveness in treating patients suffering from knee osteoarthritis and increases ROM at hip and knee joint. Isometric exercises showed better results with modified gait pattern. As compared to group A, the range of motion of the knee and hip flexion increased significantly improved in group B. As our results shows that alternative hypothesis of this study is right, which states that there is a major impact of modified gait pattern combined with isometrics exercises in patients suffering from knee osteoarthritis.
Keywords: Modified Gait Pattern, Isometric Exercises, Knee Osteoarthritis, Range of Motion
INTRODUCTION
Arthritis is probably the highest common factor of disability in the population. In the USA more than 40 million people have chronic symptoms of arthritis and the symptoms that are shown include joint pain. OA influences the 21 population in the USA. 2.1 million of the total population in the USA are diagnosed by rheumatoid arthritis and gouty arthritis [1-3]. In elderly patients the most common joint disease is knee osteoarthritis which results in increased sway of posture and impairment of balance which leads to increased risk of fall in knee osteoarthritis patients. Exercises in older patients which have knee osteoarthritis can increase balance improvement and postural sway decrease [4,5]. The older adults of age 65 mostly face the condition of osteoarthritis. Knee osteoarthritis is mostly associated with disability and increases social cost in comparison with any other joint osteoarthritis. In older adults aged 65 years approximately 30 percent have abnormalities in radiographic findings. 40 percent of the population have symptoms of associated arthritis. When this arthritis has been developed in patients, the main goal is to reduce further prognosis and prevention of the arthritis. Obesity is a high risk of osteoarthritis. Mostly risk in women which shows symptoms reduction of weight loss may be indicated [6-8]. For many decades, OA was also called the wear and tear disease, which can lead to deterioration and immobility of the joint. That is because of increasing pressure on the weight bearing joint [9].
Pain which increases during movement and gets better during rest. Swelling is most common in knee osteoarthritis patients. In the joint patients may feel warmness. Stiffness is highly common in the knee joint and is most commonly felt when the patient has been sitting for a long time or especially in the morning. The knee joint mobility is decreased which makes using the stairs, walking and moving in and out of chairs and cars tough. Crackle sound may also be audible when the patients move their affected knee [10-14].
The ratio of risk of fall in knee OA patients with unilateral joint involvement is 53% and bilateral joint involvement is 74% and those with grade 3 and 4 is 85% chances with risk of fall [15]. The initial changes occur in the articular cartilage with osteoarthritis, which then leads to changes in the subchondral bone that can be associated with the initial change so treatment that prevent it altogether could be started to reverse the disease from progressing further [16,17]. Disorders in balance and gait are more commonly found in elderly people and are one of the main causes of falls in this population. They are described by higher morbidity and death rates, as well as decreased level of function. The most usual causes include orthostatic hypotension and arthritis; however, most of the gait disorders involve multiple factors contributing to it. Many changes in gait are associated with underlying medical conditions [18]. The effect of modification of gait in knee OA patients is performed in the patients retraining. In which external knee adduction movement should be reduced. The study pays attention to the position of foot, sway of trunk, speed of walking and movement of knee in 3D. By external KAM (knee adduction movement) we increase the walking speed (17-30%) and movement of flexion (32%). Decrease in KAM not cause the slower speed of walking. KAM reduce mainly the toe-in (45%) and movement of transverse (38%) in the early stance phase in late stance toe-out reduce the KAM (56%).in early stance phase and mid stance phase KAM usually decreases (21-24%) [19].
OBJECTIVE
To identify the effects of modified gait pattern with isometric exercises on ROM (hip & knee) flexion in knee osteoarthritis patients.
HYPOTHESIS
MATERIALS AND METHODS
Study Design: Quantitative comparative study.
Study setting: The subjects were knee osteoarthritis patients with grade 3 & 4 of Kellgren Lawrence scale who were at greater risk of falling due to osteoarthritis. The half of patients received modified gait pattern along with isometric exercises and other half received isometric exercises. Government setting was Allied Hospital, Faisalabad. Private setting was Irfan medical city, Faisalabad.
Sample size: 30.
Sampling technique: simple random sampling technique was used to collect sample.
Inclusion criteria
Exclusion criteria
Procedure
Desmond risk of fall questionnaire developed by blue ridge et al. A Kellgren Lawrence scale was used to identify the grades of osteoarthritis in patients and also to collect data. A questionnaire designed in USA by Blue Ridge et al called Desmond scale for risk of fall. Isometric exercises with knee dorsiflexion, resisted knee extension in sitting, knee isometric in long sitting (Towel press). 2-5 min baseline walk for group B and ultrasonic waves for 10 min was applied on each knee joint before each treatment session. Increase toe out angle, lateral trunk lean, medial insoles and wedges. The informed consent was taken from the patients of knee OA. Before the informed consent given to the PTs, they were fully educated about the purpose of study, method and measures and only then they were asked to join the study if they are willing. Then we were given the Desmond risk of fall questionnaire by Blue Ridge et al and ask them to fill the questionnaire. The duration of data collection was 1-2 months. Overall study duration was 4 months after the approval of synopsis.
Statistical Analysis
The collected data was analyzed by using SPSS version 23. Descriptive statistics represented in the form of graph and chart. Independent sample t-test was applied for comparison between groups. Repeated Measure ANOVA was used to check the effects within groups. Significance is checked at p-value less than 0.05.
RESULTS
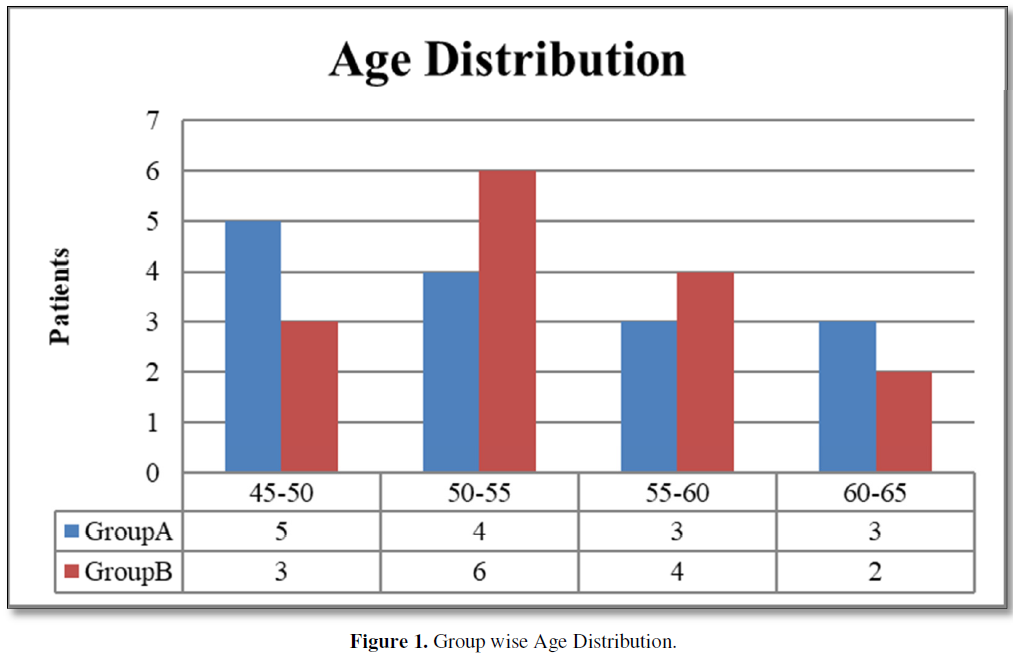
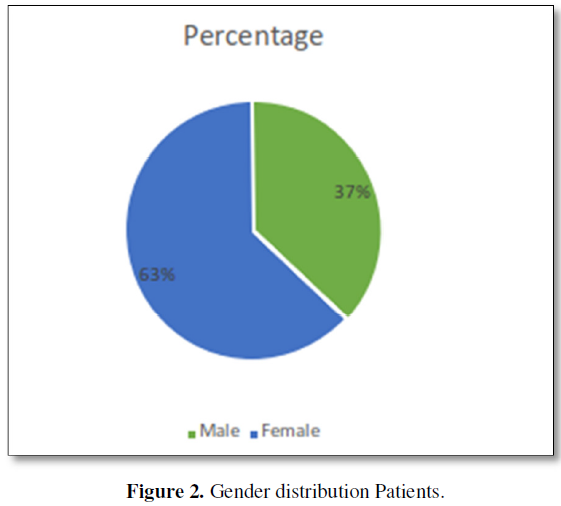
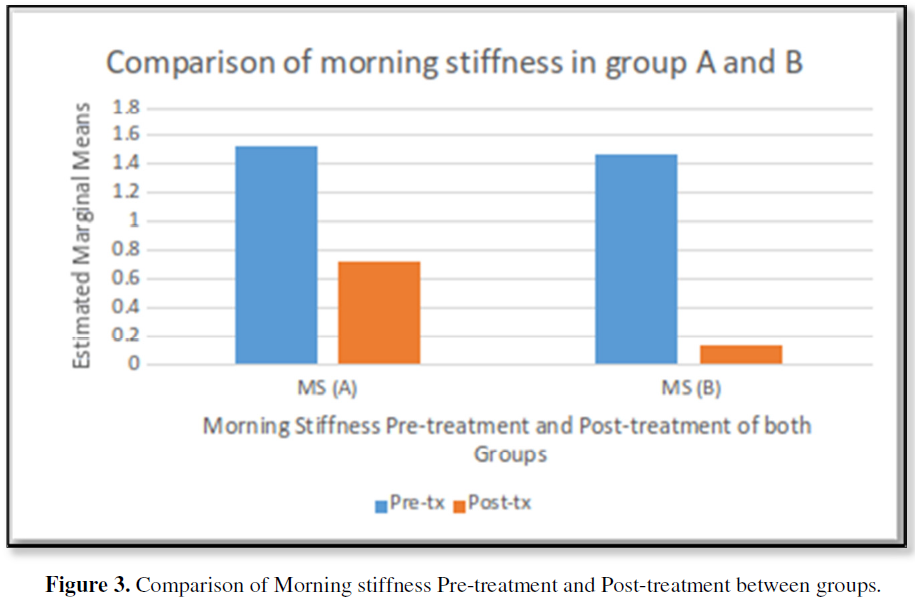
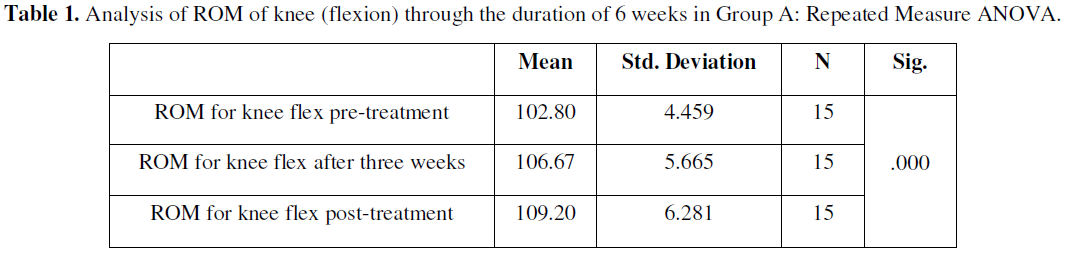
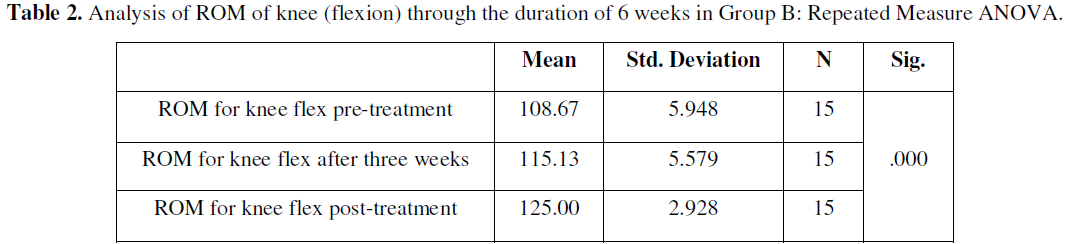
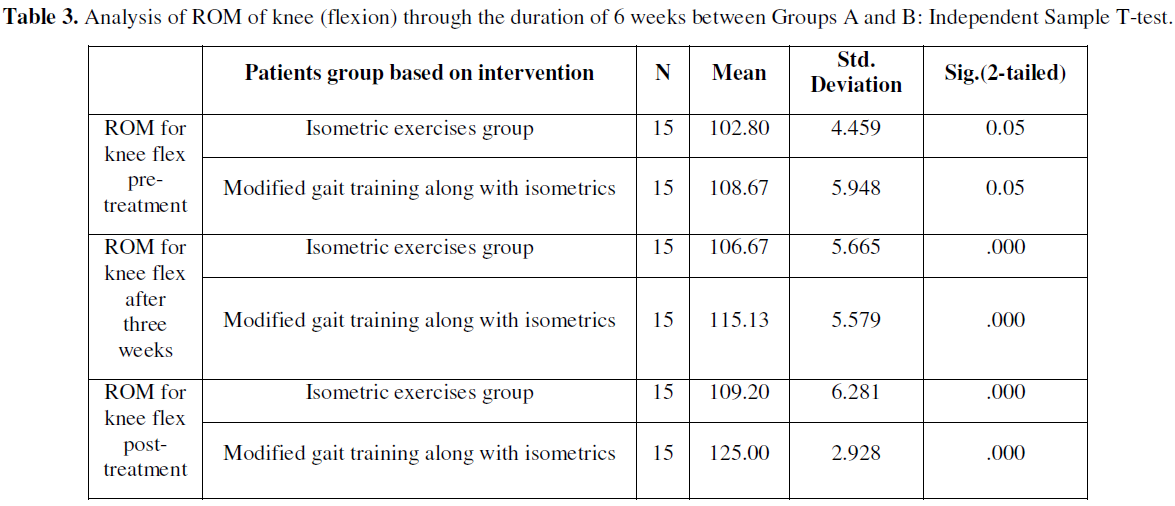
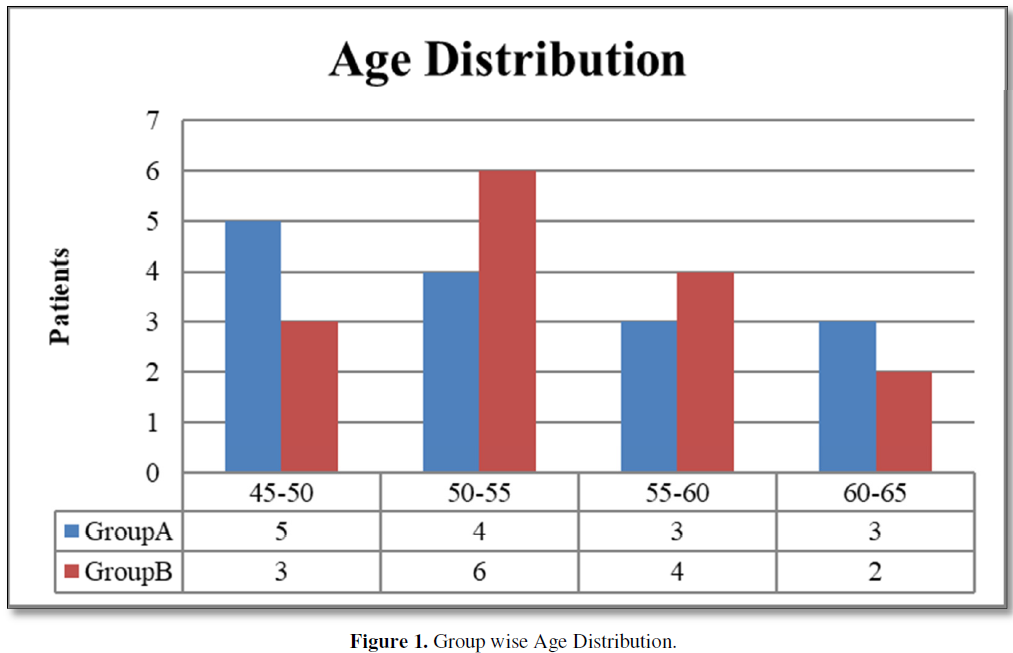
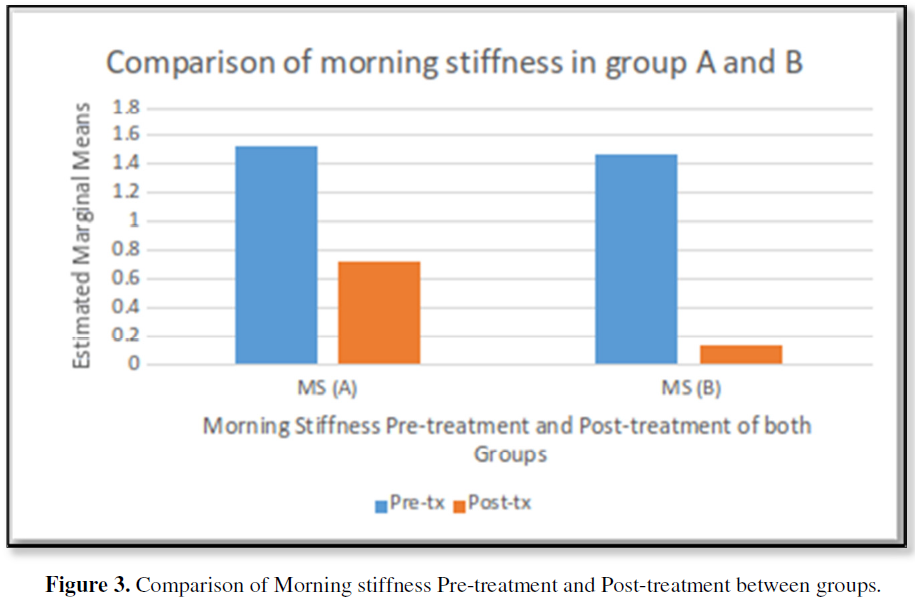
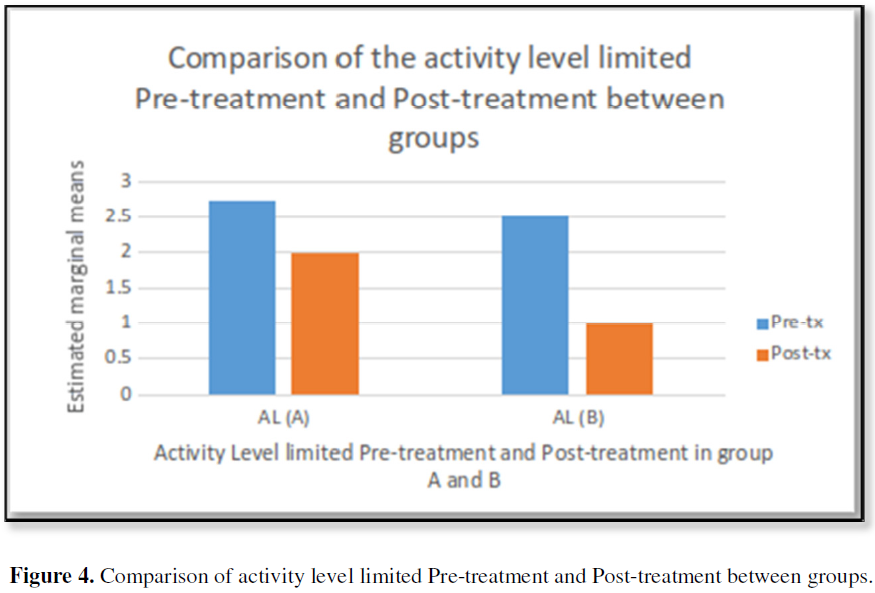
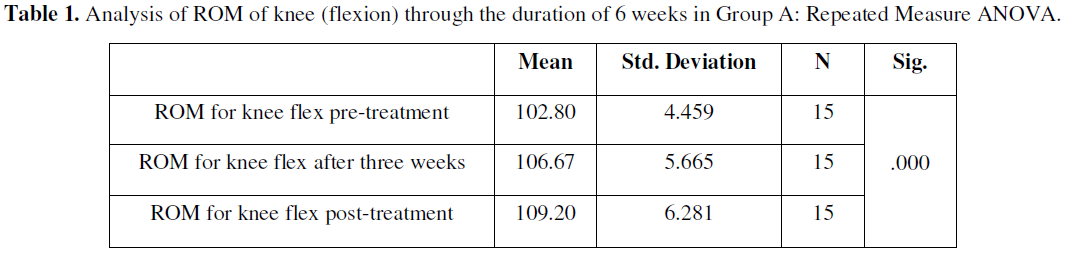
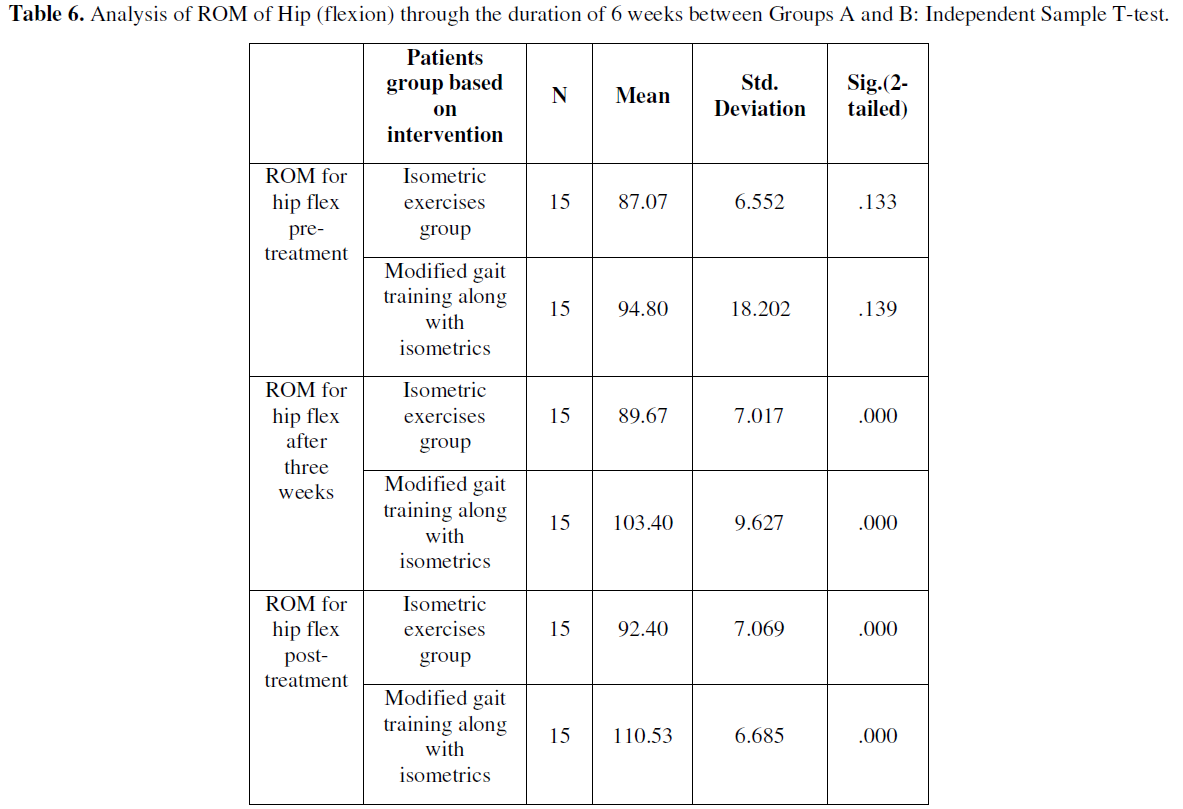
Out of 30 patients 15 were allocated on each group. Overall average ± S.D of age of patients were 55.89 ± 3.52 (Figure 1). There were 30 total participants recruited to the study. It is quite visible from the chart that maximum 63% (19) participants were from female category of gender while only 37% (11) male participants were enrolled into the study (Figure 2). It is a clear decrease in the morning stiffness of participants in group B (receiving isometrics along with gait modification) from Mean=1.47 to 0.13 as compare to the group A (receiving isometrics exercises) from Mean=1.53 to 0.73 (Figure 3). There is a significant difference of changes in the activity limitations of both groups. As group A receiving isometrics exercises show a less decline in the activity limitation level while on the other hand group B receiving isometrics along with gait modification show a more decline in activity limitation level before and after the treatment sessions (Figure 4). Above table shows that the value of p is less than 0.05 which means it is statistically significant while the mean changes from 102.80±4.459 at baseline to 106.67±5.665 at 3rd week to 109.20±6.281 at the end of treatment of participants of group A (Table 1). Above table shows that the value of p is less than 0.05 which means it is statistically significant while the mean changes from 108.67±5.948 at baseline to 115.13±5.579 at 3rd week to 125.00±2.928 at the end of treatment in the participants of group B, which is the clear indication that ROM is increasing rapidly in group B members (Table 2). There were 30 subjects taken totally into the study (Group A=15 and Group B=15) there ROM of knee flexion was taken and statistically compared between both groups at baseline, after 3rd week and at 6th week (post-treatment). Table of group statistics is showing the comparison of mean values of ROM between both groups. Independent sample t-test shows there was a significant difference of ROM of knee flexion at baseline between both groups as the (p-value =0.05) but at the last of treatment the results became statistically significant (Table 3). Above table shows that the value of p is less than 0.05 which means it is statistically significant while the mean changes from 87.07±6.552 at baseline to 89.67±7.017 at 3rd week to 92.40±7.069 at the end of treatment of participants of group A (Table 4). Above table shows that the value of p is less than 0.05 which means it is statistically significant while the mean changes from 94.80±18.202 at baseline to 103.40±9.627 at 3rd week to 110.53±6.685 at the end of treatment of participants of group B (Table 5). There were 30 subjects taken totally into the study (Group A=15 and Group B=15) there ROM of Hip flexion was taken and statistically compared between both groups at baseline, after 3rd week and at 6th week (post-treatment). Table of group statistics is showing the comparison of mean values of Hip flexion ROM between both groups. Independent sample t-test shows there was no significant difference of ROM of Hip flexion at baseline between both groups as the (p-value <0.05) but at the last of treatment the results became statistically significant (Table 6).


DISCUSSION
This research was carried out to assess the efficacy of a modified gait pattern along with isometric exercises on ROM (hip and knee) flexion in patients suffering from knee osteoarthritis and how it aids in the reduction of movement restriction. In this analysis, a modified gait pattern was compared to isometric exercises, and the findings indicate that a modified gait pattern paired with isometric exercises on ROM (hip and knee) flexion is more helpful in reducing the chance of falling than isolated isometric exercises [16-19]. Shakoor [20] conducted a study in 2010 to evaluate the effects of isometric on the reduction of symptoms related to knee osteoarthritis. They found that isometric quadriceps muscle building activity can help relieve symptoms of osteoarthritis in the knee. In current study results shows that isometric exercises have significant role in decreasing movement limitation and increasing range of motion at hip and knee but in the combination of modified gait pattern. Topp [21] conducted a study, they concluded that patients with knee OA benefit from dynamic or isometric strength exercise, which increases physical efficiency and decreases knee joint pain. Our study also shows that isometric exercises play a major role in reducing mobility restriction and increasing range of motion at the hip and knee, but only when combined with a modified gait pattern.
Booji [22] conducted an analysis in 2020 and they concluded that the most effective gait modifications for lowering knee adduction often result in a rise in co-contraction, undermining at least some of the impact on net knee load. It shows that gait modifications have significant result in gaining desired functional results in knee osteoarthritis patient. In our study results shows that group B has remarkable decline in the activity limitation due to the combination of modified gait pattern with isometric exercises which improves range of motion both at knee and hip in patients suffering from OA. Fregly [23] carried a study in 2007 on a single patient of OA to design the gate modification based specifically on the patient they concluded that using complex optimization of patient-specific, full-body gait models, this research shows that it is possible to devise novel patient-specific gait modifications with potential clinical gain. It demonstrates that gait changes have a huge impact on achieving optimal clinical outcomes in knee osteoarthritis patients. Our findings indicate that B Group has a significant decrease in movement limitation due to the combination of a changed gait pattern and isometric exercises, which increases freedom of motion at both the knee and hip in patients suffering from OA. Richards [24] conducted a RCT in 2018, they concluded that biofeedback practice to enable gait modifications are a practical and results shows immediate effects. Even so, at the time of follow-up, decreases in knee adduction moment were less noticeable in some patients, implying that a lifelong regime to improve the results of the conditioning protocol is needed to affect the development of knee osteoarthritis in the long term. In current study Group B received gait modification along with isometric exercises for the improvement of range of motion at hip and knee joint, p=0.00 which shows that significant in group B which depicts that treatment given to group B is more effective as compared to the statistical results of group A. Tok [25] conducted a study in 2011. The results of this study show that after CPM-ES combination or isometric exercise therapy, knee OA patients stability ability improved in both static and dynamic environments. The improvement may help knee OA patients from falls and increase their feelings of safety during physical exercises. It demonstrates that isometric movements, in combination with other physical therapy protocol, have an important impact on achieving optimal functional outcomes in knee osteoarthritis patients. The findings of our research indicate that group B has a significant decrease in movement weakness as a result of the combination of modified gait pattern with isometric exercises, which increases range of motion at both the knee and hip in patients with OA [25].
CONCLUSION
Modified gait pattern along with isometric exercises showed effectiveness in treating patients suffering from knee osteoarthritis and increases ROM at hip and knee joint. Isometric exercises showed better results with modified gait pattern. As compared to group A, the range of motion of the knee and hip flexion increased significantly improved in group B. As our results shows that alternative hypothesis of this study is right, which states that there is a major impact of modified gait pattern combined with isometrics exercises in patients suffering from knee osteoarthritis.
RECOMMENDATIONS


REFERENCES
No Files Found




Internationally Accepted
Share Your Publication :