
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Philip L Millstein*
Corresponding Author: Philip L Millstein, Department of Restorative Dentistry, Harvard School of Dental Medicine, Boston, Massachusetts, USA.
Received: March 10, 2026 ; Revised: March 14, 2026 ; Accepted: March 16, 2026 ; Available Online: March 17, 2026
Citation: Millstein PL. (2026) Implant Restorative Intensity Upon Occlusal Contact. J Oral Health Dent Res, 5(2): 1-4.
Copyrights: ©2026 Millstein PL. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
This paper describes various clinical situations where occlusal contacts become intense and destructive. At present there is no way to permanently record and profile occlusal health and pathology.
Keywords: Implant, Occlusal, Contact, Zirconia, Restorations
“Touch is communicated from the body to the brain, where it is perceived as sensation and used to shape behavior. Touch dysfunction can occur with chronic pain” (1). Occlusal contact intensity, clenching and bruxism may be a result of touch dysfunction. Implant placements with ceramic restorations do not exhibit touch function as do natural teeth. Dentists depend upon the mechanoreceptors in the periodontal housing to magically adjust a newly inserted restoration into occlusion. But that is impossible because too many variables are left to chance. Proprioception which allows the brain to perceive occlusal contact is minimal or non existent with implant restorations because they have no periodontal fibers (2). If a vital tooth restoration is intentionality under occluded then proprioception will not engage without actual occlusal contact (3). There is no sixth sense like in sharks where they can touch without touching (4). Sharks are attracted to minimal electrical waves which transmit the element of touch without physical contact. A pseudo sixth sense in humans allows the brain to perceive body position, movement, and force without looking (1).
Grinding and contact intensity rely on receptors in muscles, joints, and the periodontium to coordinate movement and maintain balance. A balanced or damaged bite would fit into this category. The patient does not look to sense location as long as there is a touch factor of engagement. Damage increases with grinding intensity (5).
Surface location is assured with touch sensitivity. Imagine a relatively worn dentition rubbing against zirconia implant restorations which are immovable. It is a battle of grinding surfaces where the hardest object breaks the weaker one. It is about contact intensity which increases over time. We can not measure the forces with shimstock or blue paper (6).
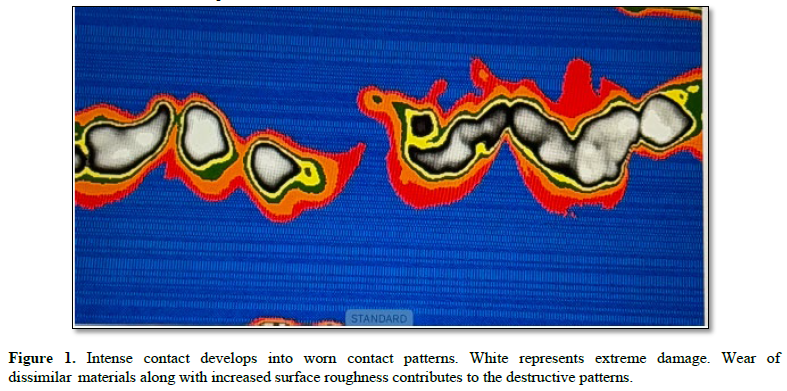
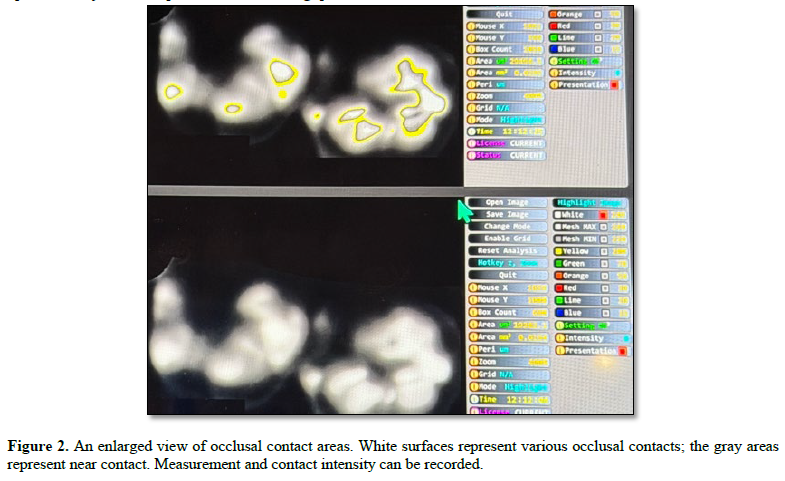
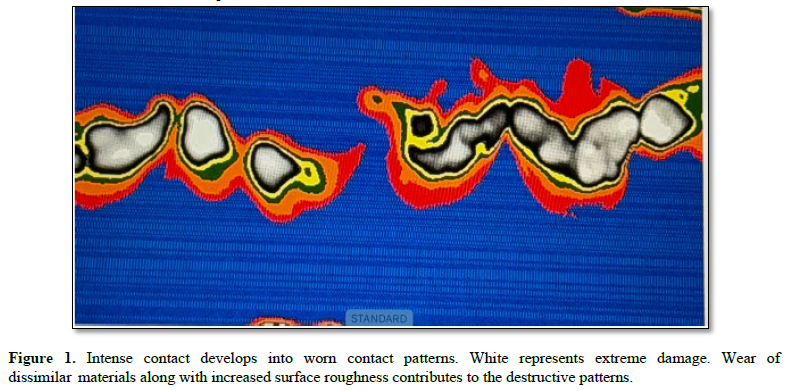
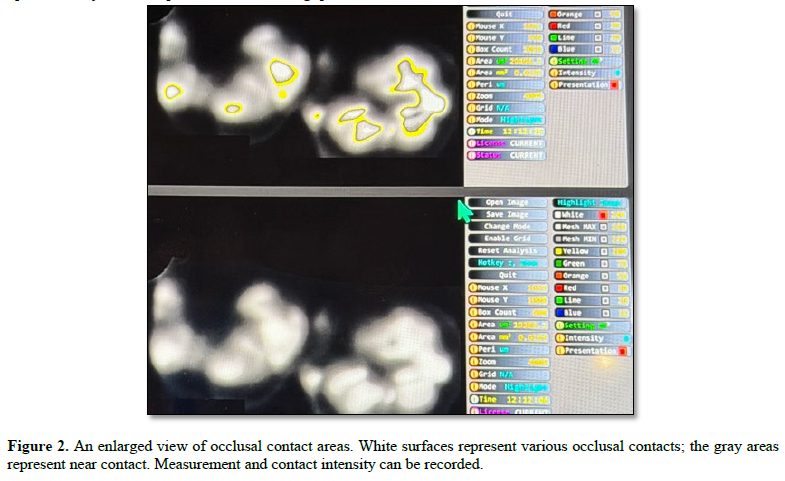
We have no marking standards nor means to measure the affects of contact intensity other than witnessing the damage afterwards Figure 2. The dentist assesses the damage and addresses the patient “my you have a strong bite let’s see what we can do.” The root cause remains unexplored and unchecked. Repairing the damage will be encouraged. Implant restorations will be suggested. This is an iterative process which goes from bad to worse. How do you break the cycle? Why do we need so many implant restorations? Why do we need so many unbreakable zirconia crowns? Is greater treatment the goal? Dentists use their tactile senses to assess light bite contact when using shim stock which is a pull through occlusal contact indicator. Touch indicators do not assess a working occlusion. There is no occlusal profile to study wear patterns. Our collective memories do not serve us well over time. Occlusal dysfunction correlates with contact intensity which has many variations. Occlusal profiles change Figure 1.
Restorative procedures alter a working occlusion. Hardened gold is a workable restorative material because it flows as it wears. The material adapts to the occlusion. Zirconia which is attractive and indestructible does not flow or adjust to a working occlusion (7). It is best to occlude zirconia restorations with care in order to minimize damage to the adjacent and opposing teeth and to adjust their occlusal contacts when required. Collective dental amnesia does not help. When the general occlusion is worn out ceramic implant restorations may become prominent and their occlusal contacts may become intense Figure 2.
Measuring light contact upon crown insertion is of little value because patients function in a working occlusion. Dentists can not assess the occlusion as it wears because they do not have an occlusal profile for comparison. There is no baseline. Simple occlusal adjustment when intense areas of occlusal contact appear can preserve a working occlusion and prevent dystrophic movement.
If a clinician does not have the simple understanding of the bio physics of a functional occlusion then he/she can not comprehend occlusal adjustment or prescribe needed repair. If a dentist does not see a whole picture of the occlusion in static and dynamic states then repair and adjustment will be limited. Understanding the meaning of touch also applies to prescribing therapeutic bite guards.
The recipient is expected to grind in the occlusal surface until the occlusion self adjusts. A balanced bite is the goal (8). Without clinical adjustments the goal may not be achieved. Many bite guards create harm or fracture because the muscles of mastication have become more powerful. Severe grinding becomes the verbal means to describe an occlusal contact profile. There is no numerical baseline for reference. What if the dentist recorded an occlusal profile upon delivery and compared the functioning profile at recall? Adjustments could be made. At present there is no baseline occlusal contact profile for the bite guard so how can a clinician assess success or failure other than by asking “does it hurt”? Is it uncomfortable? This is the best that dentists can do without an occlusal profile for reference. The science of dental occlusion has not changed in the last century. We still use untested blue paper marks to read the occlusion.
 Newer force measuring devices extrapolate their measurements from plastic wafers to working occlusal surfaces but their accuracy remains untested. There are no testing standards. Contact intensity is not measured. Touch sensitivity does not suffice as a measuring device. Shim stock is a tactile measuring indicator. We use old measuring systems that are untested to measure precise occlusal contact areas that are generated by new technologies (8). Perhaps it is time to enter the twenty first century. An impression material is used to record occlusal contact. If a patient bites hard and grinds the working occlusion is recorded. The results of clenching and grinding can be recorded and measured on a digital scan. We use a silicone impression material that does not polymerize and place it in a triple tray (9) We then inform the patient to bite hard into the silicone impression material. We have made an instant inter occlusal record which is immediately placed onto an illuminated source in an impression scanner and a picture is taken from above. The total procedure takes less than a minute. A permanent copy has been made. Using an image analysis program (Image J) a profile of the black and (white contact print is converted to a calibrated colored map for easy viewing (10)). Bite light occlusal contacts can be recorded and compared with heavy bite intense contacts. The intense affect of occlusal contacts has not been investigated. One reason is that no one understands the sciences of touch and proprioception as they relate to occlusal contact and the dental occlusion. The words occlusion and occlusal contact are used interchangeably but they have different meanings. Contact is an essential component of dental occlusion. Study clubs teach occlusion for dental practice. They do not explore the science of dental occlusion. It does not pay. Longitudinally controlled clinical studies do not exist. Repair pays. A basic understanding of touch as it relates to occlusal contact and the occlusion remains a challenge Figure 3. Solving the mystery remains a challenge.
Newer force measuring devices extrapolate their measurements from plastic wafers to working occlusal surfaces but their accuracy remains untested. There are no testing standards. Contact intensity is not measured. Touch sensitivity does not suffice as a measuring device. Shim stock is a tactile measuring indicator. We use old measuring systems that are untested to measure precise occlusal contact areas that are generated by new technologies (8). Perhaps it is time to enter the twenty first century. An impression material is used to record occlusal contact. If a patient bites hard and grinds the working occlusion is recorded. The results of clenching and grinding can be recorded and measured on a digital scan. We use a silicone impression material that does not polymerize and place it in a triple tray (9) We then inform the patient to bite hard into the silicone impression material. We have made an instant inter occlusal record which is immediately placed onto an illuminated source in an impression scanner and a picture is taken from above. The total procedure takes less than a minute. A permanent copy has been made. Using an image analysis program (Image J) a profile of the black and (white contact print is converted to a calibrated colored map for easy viewing (10)). Bite light occlusal contacts can be recorded and compared with heavy bite intense contacts. The intense affect of occlusal contacts has not been investigated. One reason is that no one understands the sciences of touch and proprioception as they relate to occlusal contact and the dental occlusion. The words occlusion and occlusal contact are used interchangeably but they have different meanings. Contact is an essential component of dental occlusion. Study clubs teach occlusion for dental practice. They do not explore the science of dental occlusion. It does not pay. Longitudinally controlled clinical studies do not exist. Repair pays. A basic understanding of touch as it relates to occlusal contact and the occlusion remains a challenge Figure 3. Solving the mystery remains a challenge.



No Files Found




Internationally Accepted
Share Your Publication :