
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Francisca Muzuka and Elison Simon NM*
Corresponding Author: Elison Simon NM, Muhibmil Univeristy of Health and Allied Sciences, Tanzania.
Received: October 13, 2023 ; Revised: October 24, 2023 ; Accepted: October 27, 2023 ; Available Online: November 17, 2023
Citation: Muzuka F & Simon ENM. (2023) Patients’ Satisfaction with Dental Services at the Muhimbili University of Health and Allied Sciences (Muhas) Dental Clinic. J Oral Health Dent Res, 3(3): 1-7.
Copyrights: ©2023 Muzuka F & Simon ENM. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
Background: Studies on patients’ satisfaction with dental services have been carried out around the world as a yardstick in determining the quality of service offered. The few studies on patients’ satisfaction with dental care in Tanzania were done many years ago and did not focus on the situation in the dental school.
Objective: This study aimed at determining the level of patients’ satisfaction with dental services provided at MUHAS dental clinics.
Materials and Methods: A cross-sectional study that involved 322 patients (or guardians, for children) attending MUHAS dental clinic. The study was carried out at the Muhimbili University of Health and Allied Sciences (MUHAS) dental clinic, Ilala district, Dar-es-Salaam region in October 2018. The study targeted all patients who attended the MUHAS dental clinics during the period of the study. Information on demographics, chief complaint, diagnosis, type of treatment, and level of satisfaction with services in the dental clinic was gathered through an interview. Every participant signed a consent form before participating in the study. Quality assurance was carried out by blindly repeating some of the participants every day of the study. Information gathered was entered into a computer and data was processed and analyzed using version 20 of Statistical Package for Social Science (SPSS). Percent distributions of respondents over the satisfaction scale were computed Chi-square was used to determine the significance of differences and multivariate multiple regression (MMR) was used to compare association.
Results: The age group 10-29 years had the highest (120) number of participants. Dental restorations were done in 113 (35%) of the patients followed by extractions in 93 (28.9%). High satisfaction levels in over 90% of the patients were scored in reception, cleanliness, and outcome of treatment. Waiting time had the highest 102 (31.7%) number of patients who were not satisfied followed by local anesthesia and cost of treatment. Above 96% of the patients responded that they would come back for treatment if need be. Over 97% responded that they would recommend the MUHAS dental clinics to friends or relatives.
Conclusion: Generally, there was a high level of satisfaction with the services offered in the dental clinics of the School of Dentistry. The aspects that showed rather high levels of dissatisfaction were waiting time followed by local anesthesia effectiveness and cost of treatment.
Keywords: Patient satisfaction, Dental services, MUHAS dental clinic
INTRODUCTION
Patient satisfaction has been investigated in many institutions because it is considered an important indicator of quality oral health care and it is a milestone of any successful dental practice [1]. Mohan [2] referred to satisfaction as patients’ emotions, feelings, and perception of delivered healthcare services while other authors defined patient satisfaction as a degree of congruency between patients’ expectations of ideal care and their perceptions of the real care received [3]. Davies and Ware viewed patient satisfaction as a multifaceted concept contributed by several factors such as; technical or the aspect of care related to the process of diagnosis and treatment, interpersonal, accessibility/availability, financial access, efficacy/outcomes, continuity of care and facilities [4].
In places that render health services, regardless of whether the service provided was of a high standard as defined by the provider if the patient is not satisfied, the service will be regarded as of little value [5]. It is, in fact, a measure of how the services provided meet the customers’ needs and expectations [6]. Zeynep reported that satisfied patients are more likely than their dissatisfied counterparts to show positive illness behaviors [7]. Where there is a poor outcome future visits to the dental practitioner for dental treatment may be delayed [8]. Burke and Croucher on their part regarded the quality of health care as the amalgamation of patients’ satisfaction and treatment outcome [9]. Patients’ satisfaction with health services is considered a measure of hospital performance, and its use has been recommended for evaluating the quality of care [10-12]. Additionally, patient satisfaction surveys have been useful in assessing a patient-centered curriculum based on the students’ interactions with patients which may guide positive changes and potentially improve the competence of new graduates [13]. To improve patient satisfaction, one is supposed to identify weaknesses and strengths in the services rendered and incorporate patient-centered approaches. Several methods have been developed to measure the quality of healthcare services. Where the results of the assessment of patients’ satisfaction are low the quality of the service must be critically examined.
In Pakistan, a study by Iqbal [14] indicated that administrative efficiency, dentist proficiency, and clinical setup are very important in enhancing patients’ satisfaction. In Tanzania, in a study conducted in public dental clinics in the city of Dar es Salaam, low satisfaction regarding patient waiting time and communication with the doctor during the procedure was reported [15]. In the same study, the cost of treatment was another area that showed low to moderate satisfaction. Further, Hiran and Masalu [16] reported patients’ satisfaction with the external environment in 98.2% of the patients in four public dental clinics in Dar-es-Salaam where adults were the most satisfied group while registration process and waiting time had the highest dissatisfaction levels [16].
In Tanzania, oral health care is provided by both public and private dental facilities. The School of Dentistry of the Muhimbili University of Health and Allied Sciences (MUHAS) dental clinic is the biggest single utility offering oral health services in the country [22]. It is a referral center and training institution for different cadres of oral health care personnel who upon qualification scatter to go and offer services in different health facilities throughout the country. It is therefore always imperative that the quality of care is monitored periodically by using different methods, among which patient satisfaction is a commonly accepted measure [11,15,16]. Most studies on patient satisfaction in this center were carried out more than nine years back [30]. Since then, several changes have been introduced with the principal aim of improving the process of discharging services to patients. Such changes included the digitalization of patients’ information systems and x-ray services, which focused on increasing efficiency and improving patient management in general.
Therefore, this study aimed to determine the current level of satisfaction among patients who attended the MUHAS dental clinic.
MATERIAL AND METHODS
This was a descriptive cross-sectional study carried out at the MUHAS dental clinic, Ilala district, Dar-es-Salaam region. The study which was conducted from October 2018 to February 2019 targeted all patients who attended the MUHAS dental clinic. Participation was voluntary whereby written informed consent was independently obtained and confidentiality and anonymity were assured. Respondents were free to refuse to participate without suffering any disadvantage. The inclusion criteria were all patients (or guardians, for children) who attended the MUHAS dental clinic and consented while the exclusion criteria were all patients who for different reasons were unable to answer questions coherently [8]. A structured questionnaire on patient satisfaction, (modified PSQ III translated into the Swahili language), which consisted of pre-coded and closed questions was used [17]. A pilot study, which included a small group of participants from the same clinic, was conducted 7 days prior to the study to pretest the data collection tool as well as training of the researchers before the actual data collection. The patients were interviewed on the same day of the visit immediately after treatment was completed and before leaving the Dental School building as has been done by others [8,10,15]. During the interview patients were requested to provide information on social demographics, chief complaint, diagnosis, type of treatment, and level of satisfaction with services received at the MUHAS dental clinic during the visit. Quality assurance was carried out by blindly repeating some of the participants every day of the study.
Information gathered was entered into a computer and data was processed and analyzed using version 20 of Statistical Package for Social Science (SPSS) [18]. The percent distribution of respondents over the satisfaction scale was computed. The age of participants was dichotomized into those below 40 years and those who were 40 years or above; social economic status into those with stable income (employed and businessmen) and those without stable income (peasants, unemployed and petty traders), education into those who had primary school education or below and those with secondary education and above and socially into those who were married or cohabiting and those who were single as was done by Kikwilu [11]. Comparisons were made and the Chi-square test was used to assess the differences with the p-value set at ≤ 0.05 and multivariate multiple regression (MMR) was used to compare association.
Ethical clearance for this study was sought from the Ethical Review Committee of the MUHAS through the Department of Orthodontics, Pedodontics, and Community Dentistry (OPCD). Permission to conduct the study was obtained from the University Authorities.
RESULTS
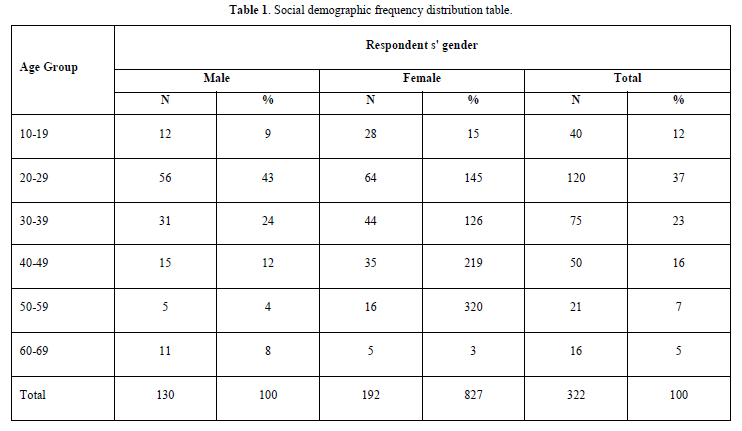
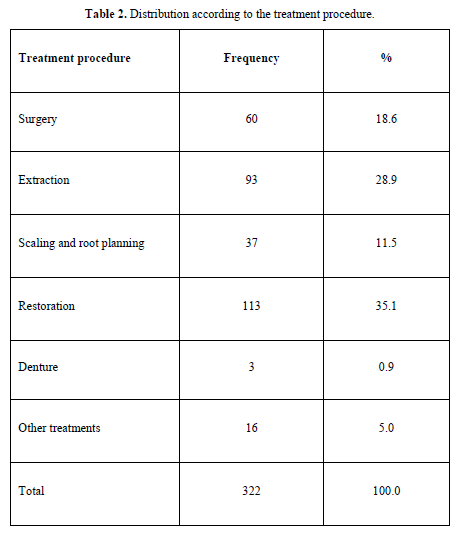
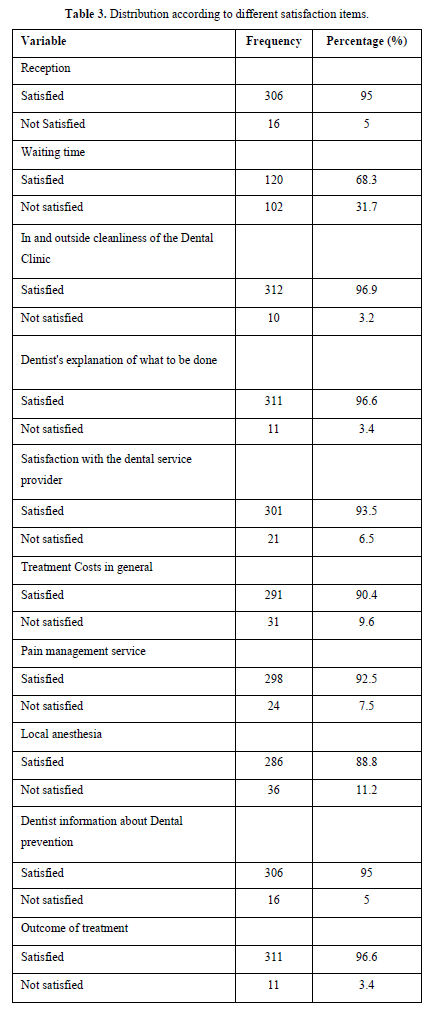
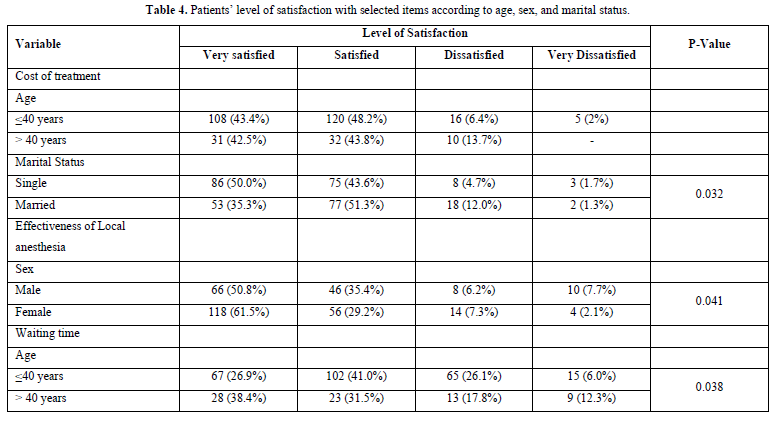
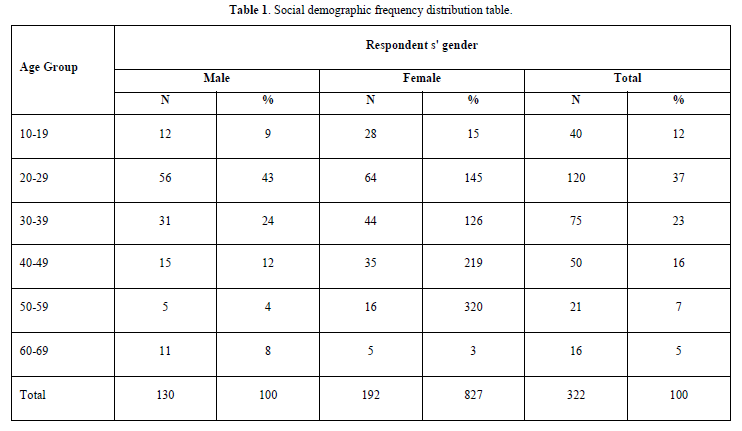
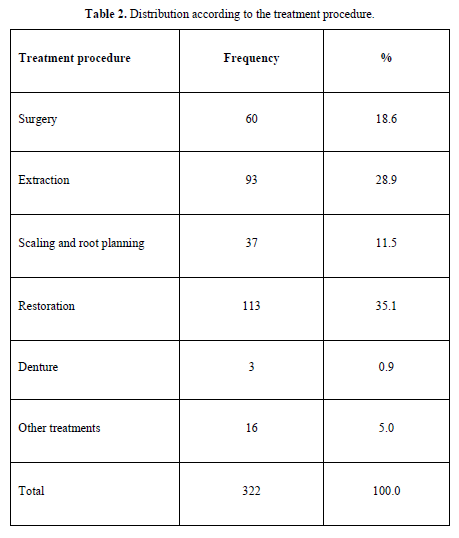
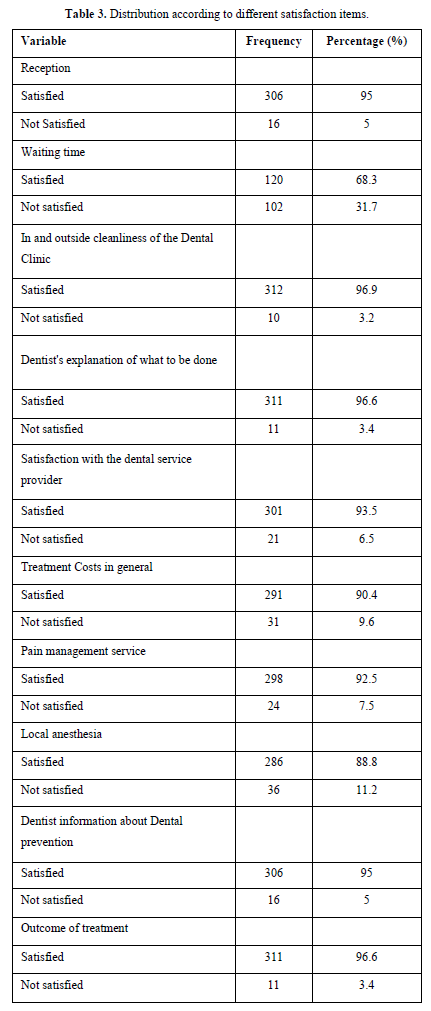
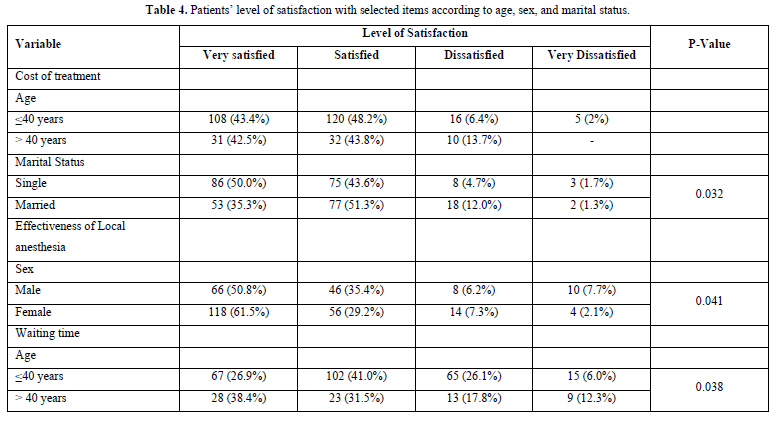
A total of 322 patients, 130 males and 192 females with an age range of 12-69 years, a mean of 32.74 and SD 12.48 were included in the study. The age group 10-29 years had the highest (120) number of participants (Table 1). Treatments that were offered included dental restorations in 113 (35%) patients, extractions in 93 (28.9%) patients, minor surgeries in 60 (18.6%) patients, and scaling/root planning in 37 (11.5%) patients (Table 2). High satisfaction levels in over 90% of the patients were scored in reception, cleanliness, and outcome of treatment. Waiting time had the highest 102 (31.7%) number of patients who were not satisfied followed by the effectiveness of local anesthesia (Table 3). Two hundred and one (62.42%) patients considered the fee for dental care as normal while 5.52% disagreed. Dichotomization along demographic lines showed that regarding local anesthesia females were more satisfied compared to males (p = 0.04). On waiting time patients who were aged 40 years and above were more dissatisfied than the younger group (p = 0.03) and on the cost of treatment patients who were married felt that it was high (p = 0.03) (Table 4).
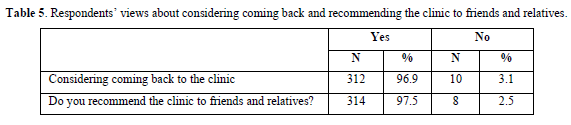
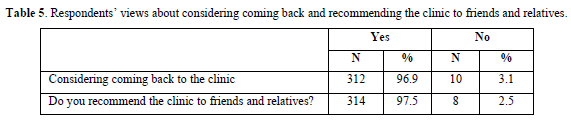
However, from a logistic regression analysis, to examine the relationship between independent variables (in this case, age, sex, education, income, and marital status) and a binary dependent variable level of satisfaction with the treatment outcome, there was no association (p > 0.05). Above 96% of the patients responded that they would come back for treatment if need be and over 97% responded that they would recommend the MUHAS dental clinic to a friend or relative (Table 5).
DISCUSSION
Satisfaction with services offered in different health facilities is a contemporary phenomenon mainly steered by the need for people to get from health providers services that meet their expectations. The instrument used in this study was a PSQ III questionnaire which was modified to suit the local situation while concurrently maintaining the important aspects regarding the accuracy of the information on the patients’ opinions [19,20]. The use of a hybrid of internally developed instruments combined with other existing standardized instruments has been advocated by others [21].
There were more females than males who attended during the study period. This is reflected in the annual records of daily attendance of patients which shows the number of females to be higher than that of males. The majority of the patients suffered from dental caries and were treated with dental restorations followed by tooth extraction (Table 2). This is very different from what was reported by Matee [15] on the utilization of dental services in Tanzania where tooth extraction was the main mode of treatment for the great majority of the patients who attended dental clinics throughout the country [22]. In the current study, other types of treatment that were offered to the patients included minor surgical procedures (apart from tooth extraction), scaling and polishing, and provision of prosthodontic appliances. Generally, similar to the findings of Hiran and Masalu [16], the highest (96%) satisfaction levels were recorded in the areas of cleanliness, the dentist’s explanation to the patients, and the outcome of treatment. This agrees with findings from the US where it was reported that courtesy and respect of healthcare providers impacted patient satisfaction while communication and explanation were seen to be the second most important aspects [23]. The high (96.6%) satisfaction levels with the dentist’s explanation to the patient, however, is contrary to the findings of Matee [15] where this area was among those that showed high levels of dissatisfaction. There was a high (95%) proportion of patients who were satisfied with reception. It is always important for the patients to get a good impression at this early stage of service delivery because it may create a positive impact in the subsequent areas where the patients will be attended in the clinics. Notably, like in previous studies by Matee [15] and Hirani and Masalu [16] in the present study, a high (31.7%) proportion of patients were dissatisfied with the waiting time. With the introduction of digitalization of patients’ information systems several years earlier, one would assume that this would no longer be a concern in the MUHAS dental clinics. This observation, however, might be attributable to the fact that the majority of patients report on an emergency basis without any appointments [11,30]. As a result, an accurate estimation of the number of patients that would be attended by a particular doctor is almost impossible leading to patients queueing for a protracted period before they are attended. Coupled with frequent interruptions in the IT system which often occur early in the morning on busy days like Mondays might have contributed to these poor scores. A relatively low satisfaction level was observed in the aspect of local anesthesia in which 11% of the participants showed dissatisfaction. This could have been attributable to the fact that in MUHAS dental clinics there are clinicians with different levels of experience [31]. The difficulties of achieving profound local anesthesia, especially in the mandibular region, as described by many authors might have led to patients feeling some pain and hence low satisfaction levels [24-26]. Females had a significantly higher level of satisfaction with local anesthesia compared to males (P = 0.04). This might reflect the fact that females tend to take good care of their teeth and therefore are used to attending dental treatment more than males. Nevertheless, so far, most available studies on the correlation between demographic factors such as age, gender, health status, and level of education with patients’ satisfaction have produced conflicting results [27,28].
Similar to the findings of Matee [15] cost was the other aspect which had a rather high (9.6%) dissatisfaction level [15]. More married patients showed a higher dissatisfaction with cost compared to those who were single (p = 0.03), possibly due to family responsibilities. Although the cost of dental treatment in Tanzania is considered to be low in comparison with other parts of the world [29], given the socio-economic status of the majority of Tanzanians it still seems to be a burden to the ordinary citizen. Patients who do not have health insurance are supposed to pay separately for registration (i.e. consultation fee), investigations (e.g. x-rays), and the treatment procedure [30]. Furthermore, some patients travel from faraway places and have to pay for transport. This most possibly led to this rather high level of dissatisfaction on the aspect of cost among the participants. Coming back for treatment in the future or recommending a relative or friend to come for treatment were among the aspects with high scores of satisfactions. This area scored very high which reflects the level of satisfaction with services in these clinics.
CONCLUSION
Generally, there was a high level of satisfaction with the services offered in the MUHAS dental clinics. Like previous studies in Tanzania, waiting time was the aspect that had a high proportion of patients who showed dissatisfaction followed by local anesthesia and cost of treatment.

No Files Found




Internationally Accepted
Share Your Publication :