
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Philip L Millstein DMD, MS*
Corresponding Author: Philip L Millstein, Department of Restorative Dentistry, Harvard School of Dental Medicine, Boston, Massachusetts, USA.
Received: June 03, 2026 ; Revised: June 05, 2026 ; Accepted: June 06, 2026 ; Available Online: June 08, 2026
Citation: Millstein PL. (2026) Treatment and Repair of a Worn Occlusion. J Oral Health Dent Res, 5(3): 1-3.
Copyrights: ©2026 Millstein PL. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
Occlusal health is generally overlooked until dental treatment is required. A plan for maintaining a working occlusion is presented and detailed.
Keywords: Occlusion, Prevention, Scanning, Printing, Appliance.
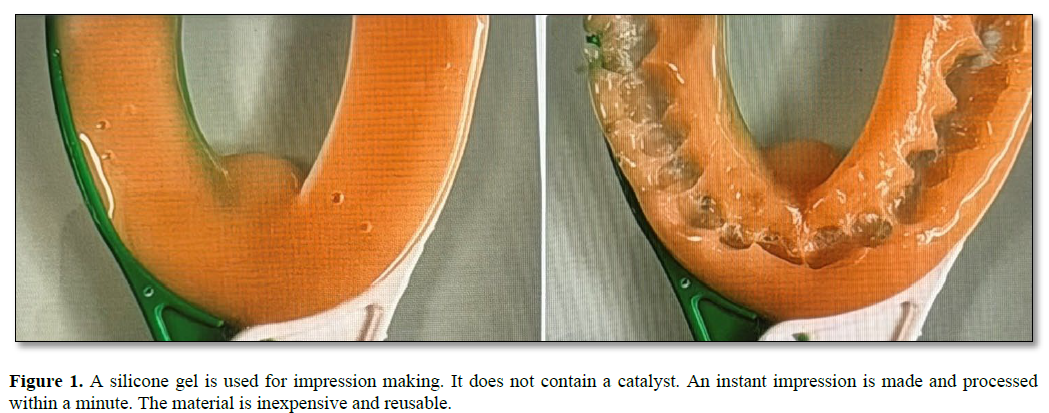
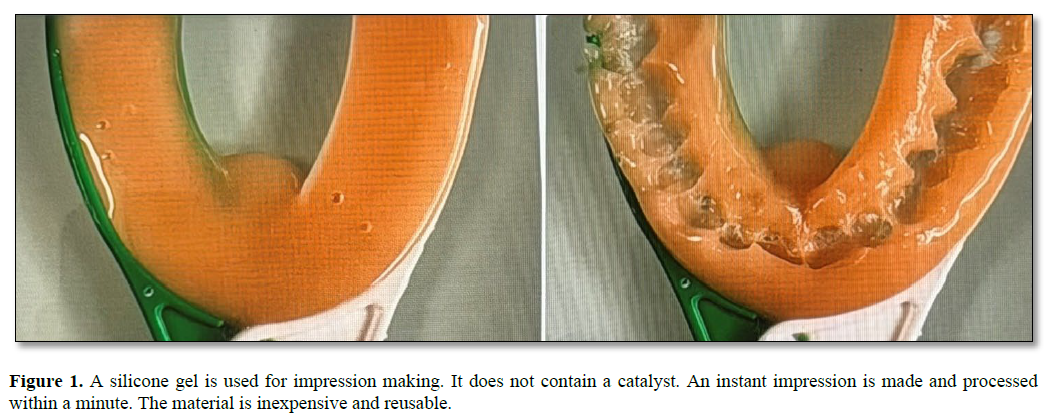
Most people survive with a worn occlusion. They don’t know it is worn nor does their dentist. A bite collapses slowly as teeth wear and occasionally break (1). Dentists repair broken teeth with zirconia crowns (2). The crowns can be made in office or commercially (3). They are easy to fit and virtually indestructible. Occlusal contact is lost (4). Posterior bite collapse is caused by a loss of posterior stops. Anterior bite collapse follows. The stops are lost. Most broken teeth are posterior teeth. Clinicians upon patient examination miss the wear dynamic as they search for broken teeth that need repair. A declining occlusion is pathological (5). It deteriorates over time as occlusal surfaces degrade. The process is irreversible. A failing occlusion affects the joint apparatus, the facial muscles, the associated nerves, the cervical vertebrae and the brain (6). This is a profound degradation and yet dentists and dental specialists pass over the occlusion in pursuit of broken teeth. Why not stabilize the bite before it breaks down and requires costly repairs? The bite can be analyzed by taking instant impressions of the inter occlusion and using the Easy Scan to determine the severity of wear which may be incremental Figure 1.
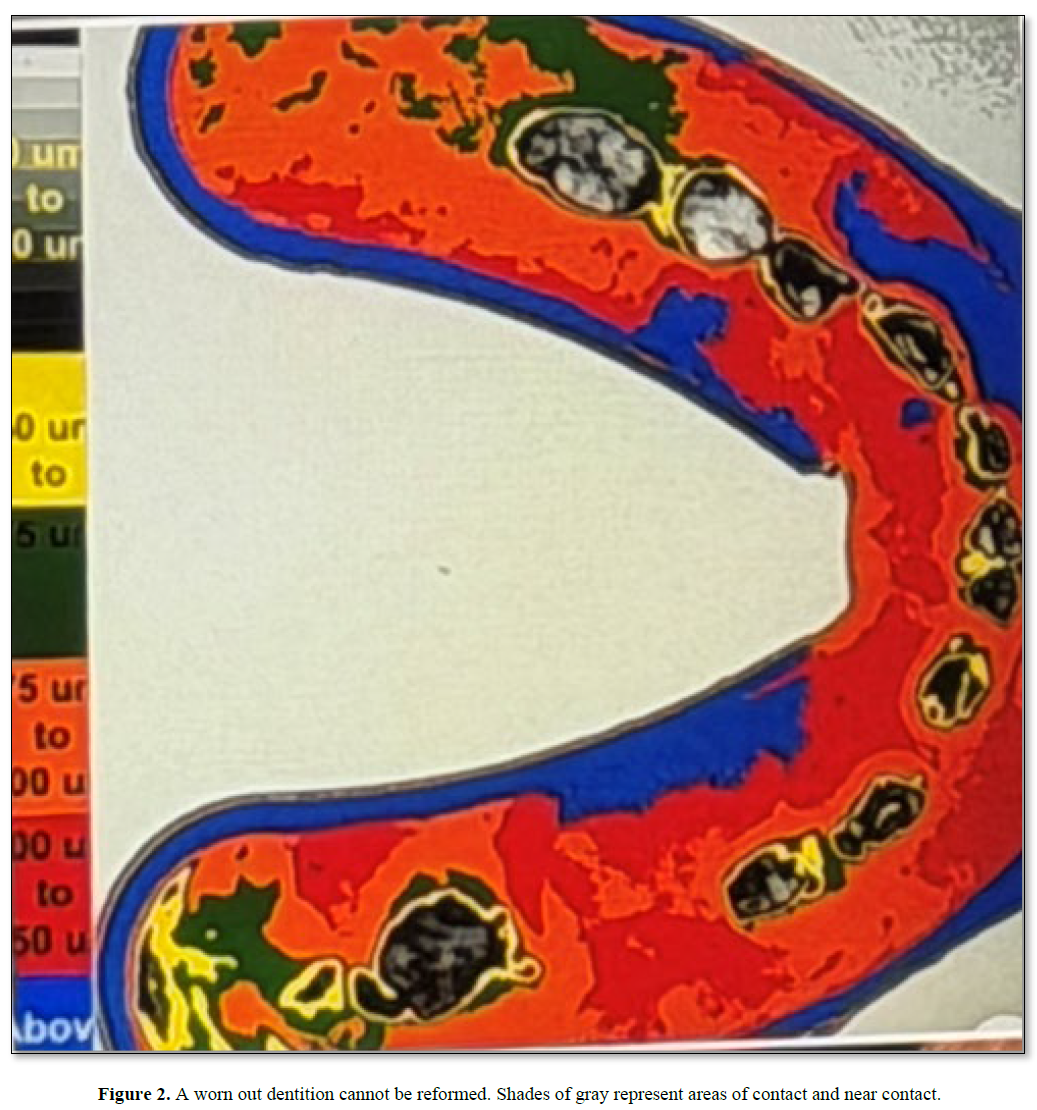
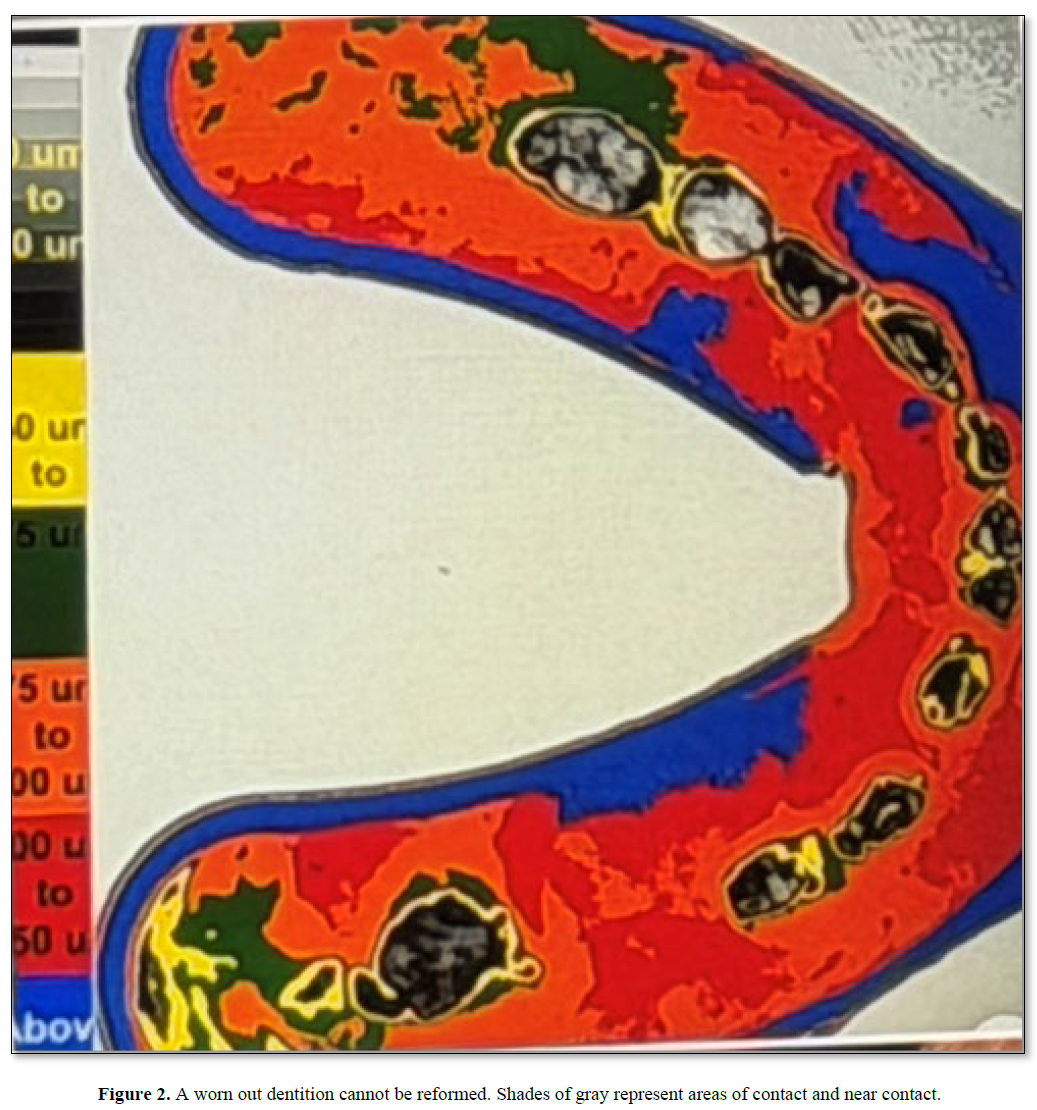
The Easy Scan is self made and is used to study the occlusion and scan occlusal contact areas. The scanning process includes illuminating, photographing and analyzing inter occlusal dental impressions using image analysis. Occlusal contacts are recorded numerically and converted to colored images (7). White is 256 pixels and represents occlusal contact. Subsequent colors represent different degrees of non contact. Shades of grey and black represent near occlusal contact which measures up to 50 microns in distance from contact. Subtle variations in occlusal contact can be visualized and numerically evaluated (8) Figure 2.
Occlusal appliances may offer a means to slow or stop grinding. They are designed and printed in office. Upper and lower digital casts and bite scans are used to design an occlusal appliance with a personalized bite pattern (9). A file is completed and the information is sent to the printer. The clinician is responsible for the surface design. Progress of occlusal disease can be monitored by evaluating wear patterns on appliances using the Easy Scan. Adjustments can be made on the appliances. A new appliance is printed when needed. Individual wear profiles differ among individuals. The proposed treatment attempts to interfere with grinding by providing graded occlusal stops. Surface gradings are selected according to the severity of occlusal wear. Success is measured on a patient to patient basis. A stabilizing appliance may slow the mandible from repetitive crushing movements. Stability is the goal.. This is not an ordinary treatment. Conventional bite guards provide a general occlusal stop. A stabilizing retainer provides stopping areas which are prescribed and upgraded as the occlusion shifts. Is it better to search out broken teeth or should clinicians provide a comprehensive oral examination which incudes the occlusion? Occlusal pathology is epidemic yet as clinicians we often do not recognize it Figure 3.

Clinical intervention should be considered. Improving the occlusion is a treatment in itself. The rhythm slows as the beat goes on (10). Reforming the occlusal profile may reduce the need for full mouth reconstructions which are physically and economically taxing. The time has come for another look at how we treat or do not treat the occlusion. The price is right. The time is now.


No Files Found




Internationally Accepted
Share Your Publication :