
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Philip L Millstein*
Corresponding Author: Philip L Millstein, Department of Restorative Dentistry, Harvard School of Dental Medicine, Boston, Massachusetts, USA.
Received: May 03, 2026 ; Revised: May 08, 2026 ; Accepted: May 09, 2026 ; Available Online: May 11, 2026
Citation: Millstein PL. (2026) The Occlusion Is an Enigma That Can Be Solved Case by Case. J Oral Health Dent Res, 5(3): 1-4.
Copyrights: ©2026 Millstein PL. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
Measuring occlusal contacts is challenging. Do the electronic systems improve upon the conventional paper marking systems?
Keywords: occlusion, contact, sensors, wafers, indicators.
An enigma is a puzzle. The occlusion is an enigma (1). What does a clinician mean by saying “I alone know what to do”? The word occlusion means to close and make tooth contact but how do we measure tooth contact? (2). As students we are taught the principles of occlusion using anatomical dental casts with ideally positioned occlusal contacts (3). We are not taught that there are many ways to judge an occlusion. A sound occlusion is built from many worn occlusal contacts that interact with one another (4). We learn the specific value of occlusal contacts in clinical practice. Sophisticated digital and electronic devices locate and record occlusal contacts (5,6,7). A practicing dentist assumes that all identified contact measurements are precise and that contact locating materials and electronic gear are factory tested and approved for clinical practice. But at present there are no government or dental association standards for evaluating the efficacy of recording systems. Do the systems do what manufacturers say they do? Is a contact location true? What should a dentist look for clinically? Clinicians assume that their work is error free but what if the measuring device they repeatedly use produces false markings or translocations? Who is to judge whether the information is accurate? If occlusal adjustments are predicated on false markings then permanent damage occurs. There is no clinical recourse. The sure way to learn about the occlusion is from other dentists and by attending short courses where outstanding dentists disclose their established procedures and products they use to be successful. A good clinician gets good results. The recommended products may work for some but not all clinicians. This is a conundrum. Test standards are needed. A product must work for most clinicians not for just a few. There are many sophisticated occlusal contact measuring devices but they are not supported by validated scientific or clinical studies. The American Dental Association posts no information in their materials testing division (8). Electronic systems record occlusal contact by using force receptors which are inserted into plastic bite wafers. The engineering efforts are evident but there is no definitive proof that the locator systems effectively locate. “It works in my hands” is not science based. A product that has been in clinical use for many years does not make it error free. Continued use enhances it’s clinical value. Some occlusal sensor systems use thin wafers with imbedded receptors to measure force (Tekscan).
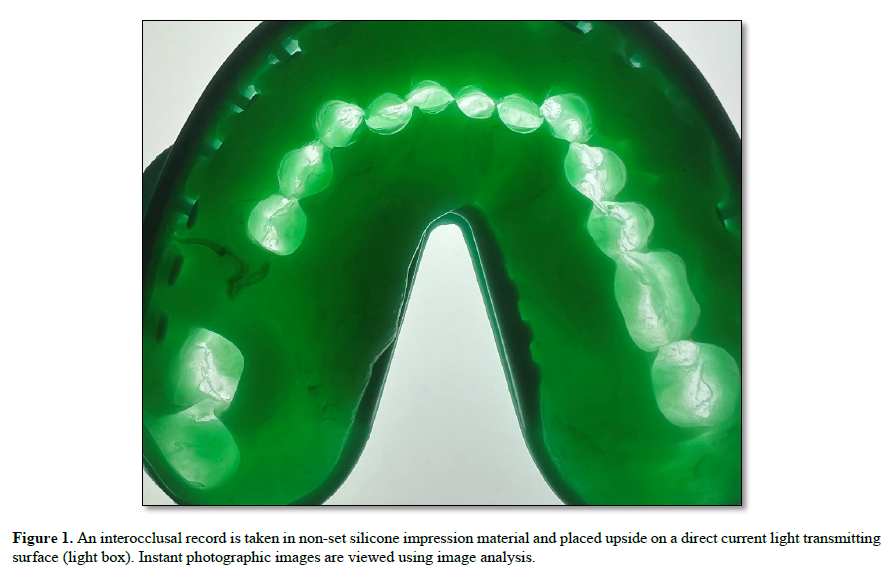
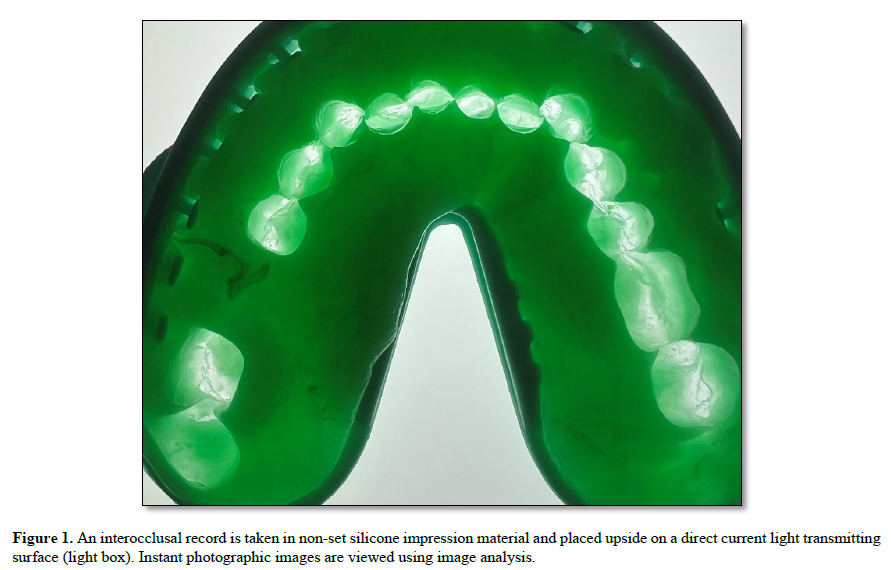
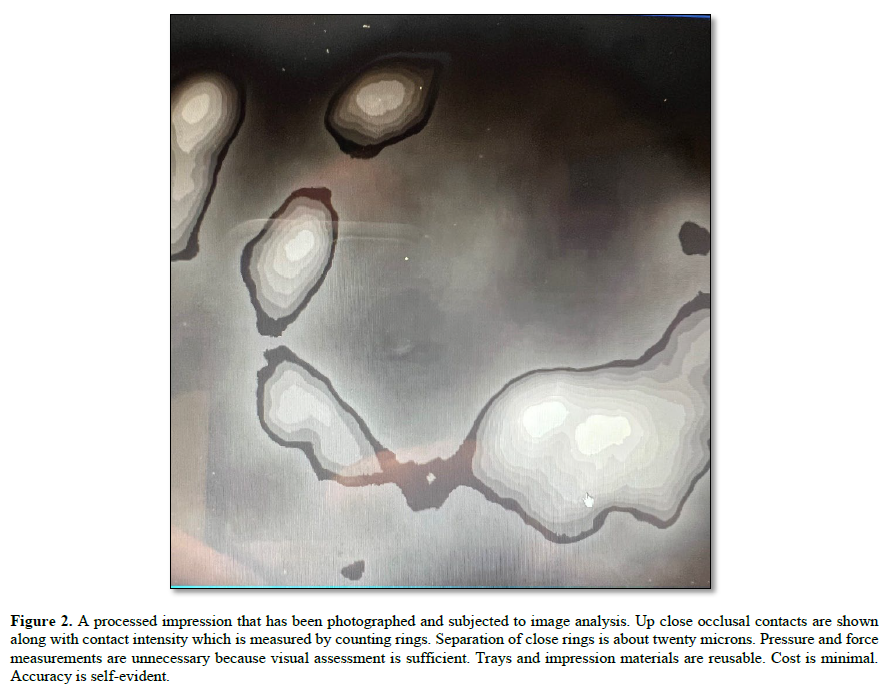
All information is extrapolated and converted into simulated occlusal contact areas. One system measures pressure and includes a marking system on the underside of a wafer (OccluSense). Again the question arises does the system locate as advertised? The retailer states that the product offers a modern approach to capturing both static and dynamic occlusion with unparalleled precision. Is this true? Are the contact markings true? Do they smudge? Is the intensity of contact recorded and are the sensor located contact areas true? No one knows. Plastic wafer systems do not freely bend and twist. When force is applied to a wafer frictional resistance occurs and the masticatory muscles react. The periodontal fibers compress (9). Each patient differs. A sophisticated measuring system adheres to manufacturing standards as shown by the accompanying wafers. The wafers record complex contact configurations of opposing tooth surfaces. Wafers with sensors record in two dimensions. Contact information is extrapolated. Impression material is not resistant to occlusal contact and full and functional closure in all dimensions is recorded (10) Figure 1. Functional recordings represent the dynamic movements that occur in closed jaw positions. Individual occlusal contact areas are a product of functional wear. Figure 2.
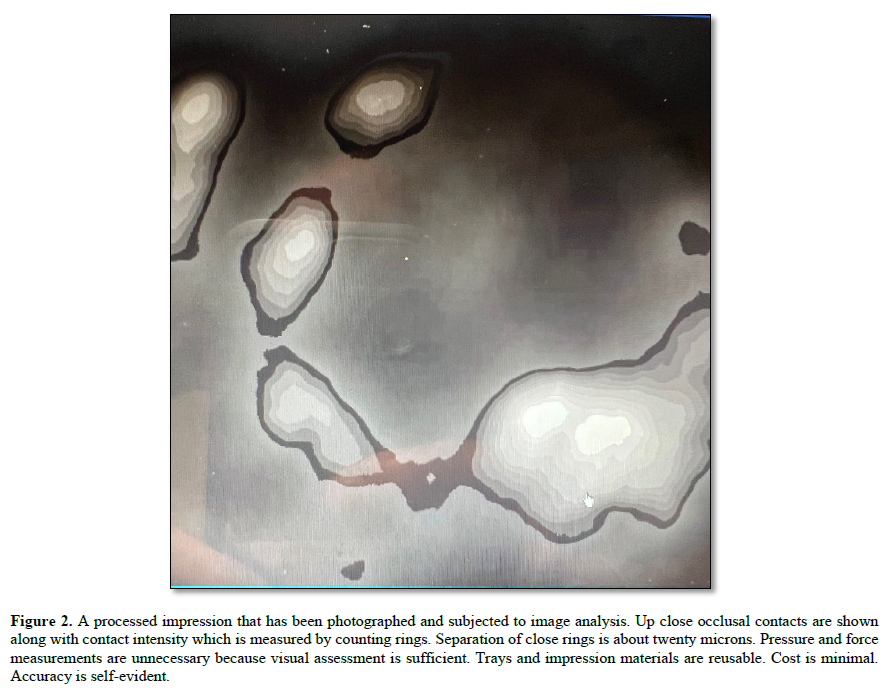
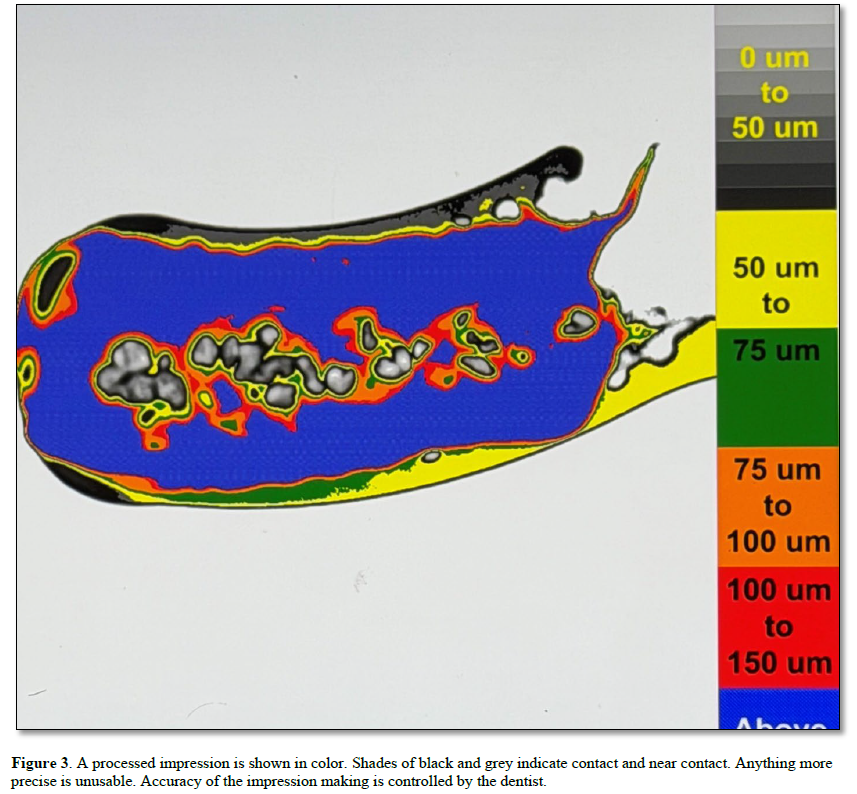
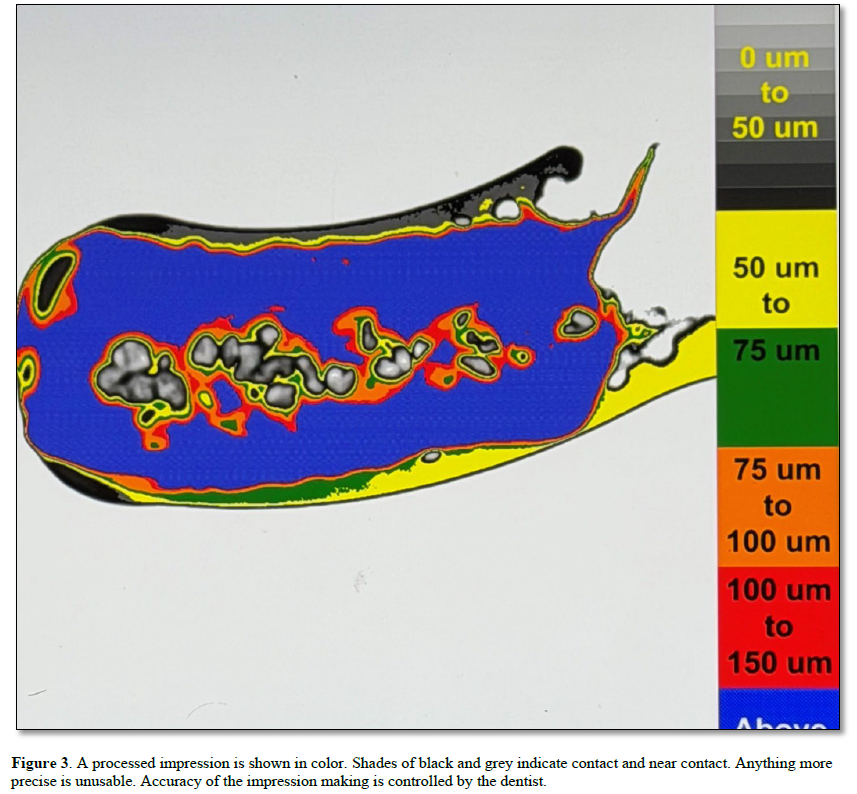
Contact information from the interocclusal record is permanent and easy to understand Figure 3. Many practitioners leave the occlusion of prosthetic replacements to the dental laboratory. The occlusal contact of restorations is mostly governed by technicians. Successful patient treatment results in little or no tooth contact? (11). The subject of occlusion is more important than what is taught in dental.school. Practicing dentists learn as they practice. Older ideas and materials are good as are newer ones. Occlusal contact is foundational to dentistry and yet we know little about it. Occlusion is a business (12).
 roducts is done by the manufacturer and not the clinician. Artists draw idealized anatomical replicas such as cusp fossae placements along with working models but reality is missing (13). Dentistry is a clinical science and yet there is little meaningful clinical research of the occlusion and of occlusal contact. Individualized tooth contacts make up the occlusion which includes jaw stability. Indiscriminate removal of occlusal contact areas is destructive. There is no way to recover lost tooth structure. Cuspal destruction is final. Do the measuring devices we use produce true and repeatable measurements? Are the resultant treatments effective? Occlusion and individualized contact are not the same because each contact is unique. All teeth make different patterns upon contact. Intensity varies. . The term occlusion is a more generalized term indicating overall occlusal contact. It is often one or two individualized contact areas that will ultimately determine whether a dentition survives or fails with time. Test and measurement remains the challenge.
roducts is done by the manufacturer and not the clinician. Artists draw idealized anatomical replicas such as cusp fossae placements along with working models but reality is missing (13). Dentistry is a clinical science and yet there is little meaningful clinical research of the occlusion and of occlusal contact. Individualized tooth contacts make up the occlusion which includes jaw stability. Indiscriminate removal of occlusal contact areas is destructive. There is no way to recover lost tooth structure. Cuspal destruction is final. Do the measuring devices we use produce true and repeatable measurements? Are the resultant treatments effective? Occlusion and individualized contact are not the same because each contact is unique. All teeth make different patterns upon contact. Intensity varies. . The term occlusion is a more generalized term indicating overall occlusal contact. It is often one or two individualized contact areas that will ultimately determine whether a dentition survives or fails with time. Test and measurement remains the challenge.

No Files Found




Internationally Accepted
Share Your Publication :