
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Philip L Millstein*, Jan Rozen, Carlos E Sabrosa and Wai Yung
Corresponding Author: Philip L Millstein, Department of Restorative Dentistry, Harvard School of Dental Medicine, Boston, Massachusetts, USA.
Received: January 26, 2026 ; Revised: January 28, 2026 ; Accepted: January 29, 2026 ; Available Online: January 30, 2026
Citation: Millstein PL, Rozen J, Sabrosa CE & Yung W. (2026) The Intensity of Occlusal Contact Patterns Reflects a Damaging Pattern of Wear. J Oral Health Dent Res, 5(2): 1-3.
Copyrights: ©2026 Millstein PL, Rozen J, Sabrosa CE & Yung W. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
This paper presents a means to adjust the occlusal contact of a restored endodontically treated tooth so that the crown can effectively move into a preset functional occlusal scheme.
Keywords: Endodontics, Restoration, Occlusion, Occlusal contact, Proprioception
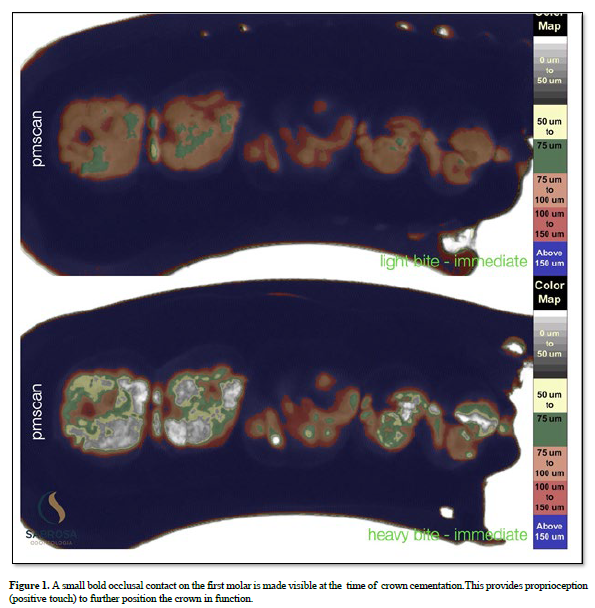
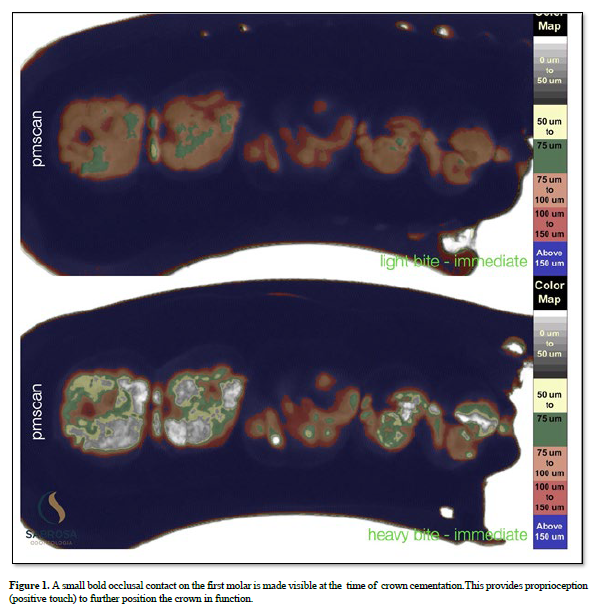
An occlusal stop often referred to as a centric stop takes place upon tooth contact. There are many stops in the posterior occlusion. They hold the mandible in position and make efficient mastication possible (1). The occlusion becomes unstable if dentists advocate removing stops while restoring teeth. Removing stops insures less trauma on new restorations. The mandible will slide forward if two or three stops which are referred to as holding cusps are removed (2). To offset the loss of contact the dentition is ground down by the patient in an attempt to stabilize the bite. If the anterior teeth remain stable then the sliding stops; if not the anterior teeth loose their guidance. Stability cannot occur because there are no holding cusps. The dentist upon routine examination looks and says “we will wait and see” and prescribes a night guard for the all day, all night, grinding. Endodontically treated teeth maintain a diminished sense of touch upon occlusal contact because the nerve plexus has been removed (3). The mechano-receptors in the periodontal housing remain active but their effect is diminished (4). Touch in humans can only occur if there is physical contact (5). Each tooth has it’s own sensory system. If a restoration has no occlusal contact then the occlusal contact areas of the adjacent teeth will shift (6) Closing forces on the teeth will become uneven. To regain occlusal balance a patient will self adjust (7). A non alignment of the teeth may follow with a pseudo positioning of the closed jaws along with a slight loss in vertical dimension. Under occluding a restored tooth is known as “ditching”. There is no occlusal contact. There is an assumption that the restoration will rise into a functioning occlusal position but that is unproven. If some actual physical contact is programmed into the occlusal profile at the time of crown delivery then occlusal contact will be assured and self adjustment will take place over time (8) Figure 1. It will never be ideal but it will be functional. The only means to record the occlusal contact areas with their various intensities is by using a recording scan which is linked to an image analysis program (Image J). Heavy and light closures of a patient are recorded using a silicone impression material in a quadrant triple tray (9). The set impressions are individually placed on an illuminated light box which is positioned six inches below a fixed camera which is connected to the image analysis program. Images are digitized and converted to color and displayed on a computer screen. The digitized records are permanent and can be used at a later time for reference. The dental materials we choose for the under structure and crown restoration are significant factors for longevity. There is no clinical research that provides guidance on the choice of restorative materials. Bench top studies offer minimally constructive information. Ultra hard materials such as zirconia are inexpensive and indestructible. They can be milled at the chair. When articulated against an opposing tooth the weaker tooth structure will fracture. Softer materials such as resin reinforced composites are a good substitute but in function they lose their occlusal anatomy. Gold is a proven material but it is costly and cannot be milled. As to restoring the understructure there is little if any substantial clinical research. It is all speculative. Perhaps what is missing in this story is planning before or after treatment. How will this treated tooth be restored? What materials for the under structure and superstructure will be employed?
What type of occlusion will be advocated? Who will decide, the restorative dentist, the endodontist, or both? The restoration is as important as the root treatment. The occlusion is a significant factor. Success depends on collaboration. Failure is a non starter.

No Files Found




Internationally Accepted
Share Your Publication :