
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Philip L Millstein*, Carlos Eduardo Sabrosa and Wai Yung
Corresponding Author: Philip L Millstein, Department of Restorative Dentistry, Harvard School of Dental Medicine, Boston, Massachusetts, USA.
Received: July 25, 2025 ; Revised: September 22, 2025 ; Accepted: September 25, 2025 ; Available Online: September 26, 2025
Citation: Millstein PL, Sabrosa CD & Yung W. (2025) Occlusal Profiles in Mixed Implant Dentitions. J Oral Health Dent Res, 5(1): 1-2.
Copyrights: ©2025 Millstein PL, Sabrosa CD & Yung W. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
This paper describes a means to create an occlusal profile that includes all jaw positions in closed contact. Occlusal contacts, intensity of contact and wear patterns are addressed.
Keywords: Occlusal contact, Implants, Contact intensity, Occlusal profiles
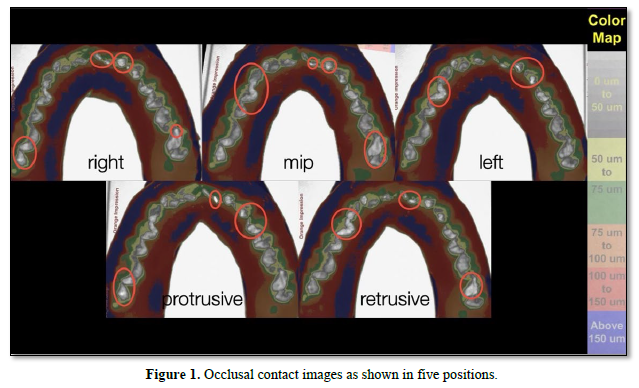
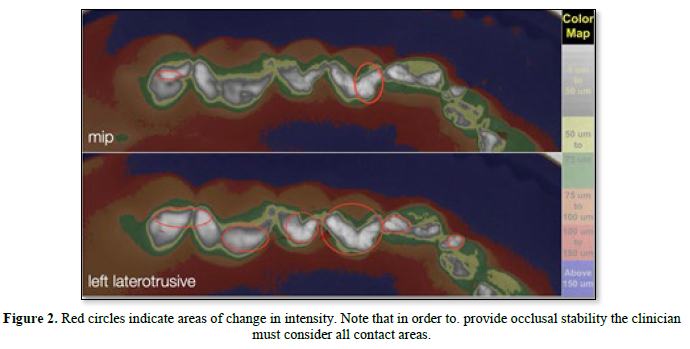
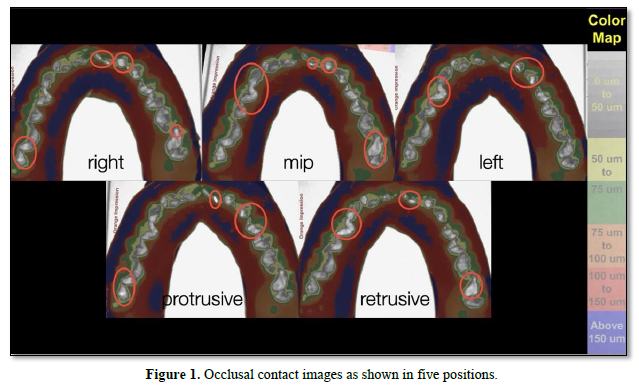
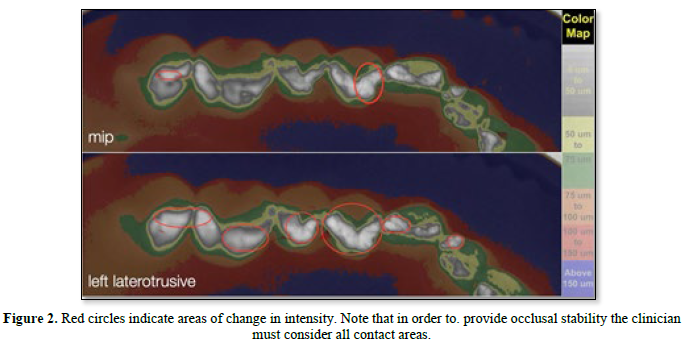
A profile is an outline of a visible object. We use five profile pictures to describe an occlusion of a working case. The five occlusal jaw/tooth contact positions are: central, left lateral, right lateral, protrusive and retrusive. These positions represent the occlusal contact border movements that all people exhibit in chewing and movement exercises. Contact positions are important because they dictate jaw movement in a closed position. That is where we chew, grind and clench. This short paper exhibits a means to profile occlusal contact jaw positions and their movements in their respective closed jaw positions. Static occlusal contact positions and dynamic contact positions are recorded and referred to periodically to assess one’s occlusal health. Changes in occlusal contact size, shape, location, or intensity may signify a pathological situation. We use a triple tray and a non-set reusable instant silicone gel material to extract intra oral contact information [1]. The flow properties of the impression material allow us to record tooth contact as it applies to jaw movement in a closed position. We process the impression using a light box to trans illuminate the impression at a fixed distance from the camera and image analysis (Image J) to process the information so that we can measure occlusal contact position, surface area, and contact intensity upon closure [2]. It is clearly visible that each profile of five jaw positions is unique as are jaw movements related to the occlusal contact areas (Figure 1). Occlusal equilibration or adjustment should include all parameters of movement [3]. Contact study includes viewing the intensity of contact along with the many wear facets and worn areas associated with grinding, eating and closed jaw movement (Figure 1). An enlarged view of a left lateral movement is also included to emphasize contact intensity that may occur upon excursive movement (Figure 2). Implants do not have a periodontium to adjust to occlusal forces therefore recording occlusal contact intensity becomes significant. Prematurities that interfere with various movements can be highlighted and adjusted to blend in with the mixed dentition. Wear and wear patterns can be assessed. The variation in biting surfaces and intensity of the bite add to the complexity of providing a balanced occlusion [3]. There is no alternative means to record changes in intensity. The use of an impression material assures repeatable closures [4]. Digital procedures do not use impression materials so positional movements upon full closure may vary along with changes in intensity. Recording movement and intensity of closure with an impression gel material provides a unique procedural change in how we assess the occlusion [5]. Contact intensity is not included upon dental examination [6]. Using a colored silicone gel to record intensity is unique because as force upon closure increases so does the increase in intensity as shown in the images. The greater the opposing force on occlusal contact the thinner the gel becomes and light transmission increases which is recorded in the occlusal images. Intensity of occlusal contact is not indicated using conventional methods. Adjusting an occlusion without a baseline is common practice [4]. Occlusal marking devices are not tested for accuracy. Intensity of contact is an unknown. More clinical research of occlusal contact indicators is needed along with ADA standards to determine the veracity of occlusal contact marking devices.

No Files Found




Internationally Accepted
Share Your Publication :