
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Nameirakpam Chingkheinganbi, Monika, Aman Arora, Viram upadhyaya and Chandrama*
Corresponding Author: Chandrama, Swami Vivekanand Subharti University, Meerut, UP, India.
Received: September 19, 2025 ; Revised: September 22, 2025 ; Accepted: September 25, 2025 ; Available Online: September 26, 2025
Citation: Chingkheinganbi N, Monika, Arora A, Upadhyaya V & Chandrama. (2025) Digital Smile Design for Aesthetic Rehabilitation: A Case Report. J Oral Health Dent Res, 5(1): 1-4.
Copyrights: ©2025 Chingkheinganbi N, Monika, Arora A, Upadhyaya V & Chandrama. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
Digital Smile Design (DSD) is an innovative approach in aesthetic dentistry that integrates advanced digital technologies into treatment planning. Unlike traditional methods, DSD uses computer-aided design (CAD), computer-aided manufacturing (CAM), intraoral scanning, and 3D imaging to create personalized smile designs that enhance precision and predictability. This method allows for detailed analysis of facial features, dental morphology, and occlusion, improving communication among patients, dentists, and technicians.
This case report highlights the rehabilitation of a patient with unaesthetic crowns, employing digital smile mock-ups, precise tooth preparation, and CAD/CAM-fabricated lithium disilicate crowns. The digital workflow enhances accuracy and patient involvement, resulting in a natural and harmonious smile.
DSD offers benefits such as reduced treatment time, enhanced visualization, and improved treatment outcomes. Despite challenges like high costs and technical demands, its ongoing integration with emerging technologies like artificial intelligence and augmented reality promises to expand its clinical applications.
Keywords: Digital smile design, Aesthetic dentistry, CAD/CAM, Smile rehabilitation, Personalized treatment, Prosthodontics
INTRODUCTION
Digital Smile Design (DSD) has revolutionized aesthetic dentistry by integrating digital technology into treatment planning, allowing for precise and predictable smile enhancements. Unlike traditional methods such as manual wax-ups and two-dimensional photographic assessments that rely heavily on subjective analysis, DSD deploys advanced digital tools including computer-aided design (CAD), computer-aided manufacturing (CAM), intraoral scanning, and 3D printing to provide an individualized, patient-centered approach to smile transformation [1]. Aesthetic smile analysis influences facial harmony, social acceptance, and self-confidence; DSD facilitates systematic assessment of facial proportions, dental morphology, gingival architecture, and occlusion through photographic and videographic records, which improves diagnostic accuracy and clinician-patient-technician communication [2].
The concept of smile design can be traced back to ancient civilizations like the Phoenicians and Etruscans who utilized carved animal tusks for dental restorations. The modern evolution of aesthetic dentistry includes porcelain veneers, adhesive dentistry, and CAD/CAM technology culminating in Dr. Christian Coachman's introduction of Digital Smile Design in 2007, offering a comprehensive digital toolset for diagnosis, planning, and patient engagement [3]. The integration of facial analysis, digital mock-ups, and minimally invasive restorative techniques in DSD enhances clinical precision and patient satisfaction.
CASE PREPARATION
A 52-year-old male patient presented to the Department of Prosthodontics and Implantology, DAV Dental College, Haryana, India, with a chief complaint of unaesthetic bulky crowns and dissatisfaction with his current prosthetic restorations. The patient requested a natural and aesthetically pleasing smile. The Digital Smile Design concept was explained, highlighting its advantages in improving treatment communication, visualization, and predictability.
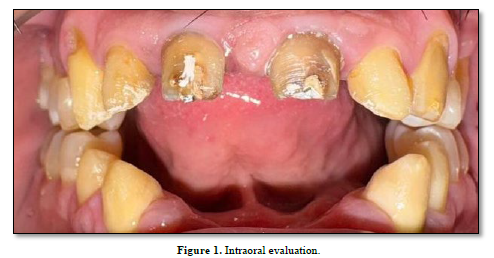
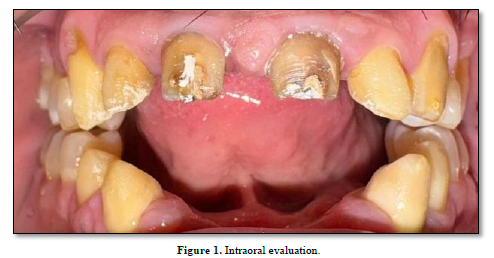
Standardized clinical photographs were taken using a Canon EOS 5D Mark IV DSLR camera with a 100mm macro lens and ring flash to obtain consistent intraoral (Figure 1).
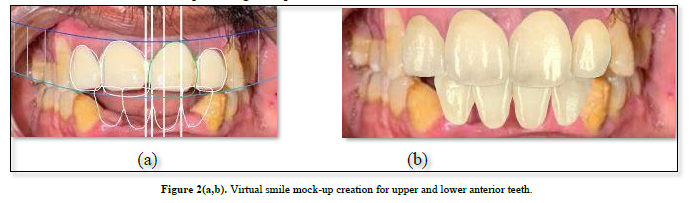
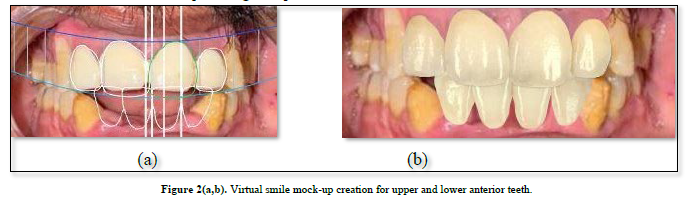
Diagnostic impressions were made using a polyvinyl siloxane impression material (Aquasil Ultra, Dentsply Sirona) for high-fidelity model fabrication. Photographs and impressions were forwarded to a Digital Smile Design laboratory, where virtual smile mock-ups for the upper and lower anterior teeth were developed using 3Shape Smile Design Software (3Shape A/S, Copenhagen, Denmark). These designs incorporated facial landmarks for accurate symmetry assessment (Figure 2a). The patient evaluated the digitally proposed smile design and gave informed consent to proceed with treatment (Figure 2b).
TREATMENT PLANNING
Removal of Existing Prosthesis and Clinical Assessment
The existing over-contoured and ill-fitting prostheses were carefully removed to allow detailed clinical examination. Findings included bilateral Angle’s Class II malocclusion, anterior open bite, and missing teeth numbered 16, 26, 31, 32, 41, and 42. These anatomical issues contributed to aesthetic imbalance, occlusal instability, and impaired mastication.
Endodontic Therapy and Tooth Preparation
Root canal treatment (RCT) was performed on teeth 13, 21, 22, and 23 using rotary NiTi files (ProTaper Gold, Dentsply Sirona) and biocompatible sealers (AH Plus, Dentsply Sirona) to resolve any endodontic pathology before prosthetic intervention. Tooth preparations for full-coverage crowns were completed on teeth 11, 12, 13, 21, 22, 23, 33, 34, 43, and 44. This preparation corrected the previous lack of tooth reduction that caused bulky crowns and compromised aesthetics.
Secondary abutments were prepared on teeth 34 and 44 to improve retention and optimize occlusal load distribution. These preparations were essential for the long-term stability of the prosthesis.
Provisional Occlusal Rehabilitation
A flexible removable partial denture (RPD) fabricated with Valplast thermoplastic material was provided for edentulous regions at teeth 16 and 26. This RPD ensured temporary occlusal support, functional comfort, and adequate retention during the interim phase. Implant placement was planned subsequently to restore permanent function and esthetics in these posterior regions.
Digital Workflow and Smile Design Protocol
Intraoral digital scans were obtained using the Trios 4 intraoral scanner (3Shape) alongside high-resolution photographic records. Patient demographics included age and gender, with tooth shade selection based on the Vita Classical Shade Guide: shade C1 for teeth 11, 12, 21, and 22, and shade C2 for tooth 13 to harmonize with adjacent structures.
The 3Shape Smile Design Software was utilized for comprehensive digital planning. Facial measurements employed the interpupillary line as a horizontal reference and the facial midline as a vertical guide, ensuring symmetry and proportional tooth positioning. The software’s tooth library allowed customization of tooth shape, size, inclination, position, and gingival margin contours for ideal integration with the patient’s facial features.
Occlusal plane correction addressed the anterior open bite, with incisal edge position tailored to dynamic lip movements for natural visual balance. Advanced 3D rendering enabled simulation of enamel translucency, texture, and surface characteristics to replicate natural aesthetics.
The finalized digital smile model was sent for fabrication of full-contour lithium disilicate crowns (IPS e.max CAD, Ivoclar Vivadent) via CAD/CAM milling (Ceramill Motion 2, Amann Girrbach), chosen for their optimal balance of strength and optical properties.
Clinical Try-In and Cementation
Try-in sessions utilized dental operating microscopes for margin fit verification and articulating paper to confirm occlusal harmony. Occlusal adjustments and polishing optimized crown integration. Final cementation used dual-cure resin cement (Variolink Esthetic DC, Ivoclar Vivadent) following strict protocols to secure durable adhesive bonds.
Treatment Outcome
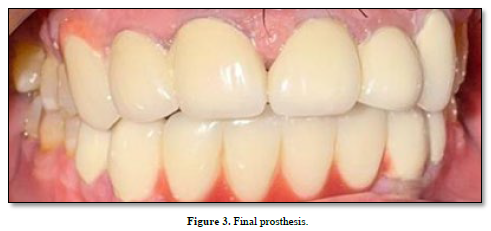
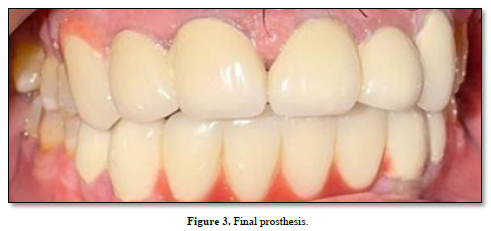
The comprehensive management integrating endodontics, digitally guided restorations, provisional occlusal rehabilitation, and CAD/CAM fabrication resulted in a functional, stable, and aesthetically harmonious smile. The patient reported high satisfaction and improved confidence (Figure 3). The digital workflow facilitated patient visualization and participation in treatment decisions, fostering trust and acceptance.
DISCUSSION
The integration of digital workflows like DSD has transformed traditional prosthodontics by improving diagnostic precision, reducing procedural errors, and shortening treatment duration compared to manual techniques [4]. The 3Shape Smile Design software offers real-time 3D visualization, incorporating facial scanning and intraoral digitization, enhancing treatment predictability [5]. However, its proprietary system limits interoperability with some third-party scanners and milling units [6]. Open-source alternatives like Exocad offer broader compatibility but lack advanced facial analytics, making them less suitable for high-esthetic cases [7].
The ability to previsualize and modify smiles digitally empowers patients, increases treatment acceptance, and reduces chairside modifications. Limitations include high initial investment and a learning curve to master software and digital equipment [8]. Conventional treatments such as fixed partial dentures or composite veneers do not provide the same level of customization or integration, making DSD preferable for complex cases with malocclusion and multiple missing teeth [9].
Future directions involve artificial intelligence and the integration of augmented and virtual reality to enhance design efficiency, improve patient interaction, and broaden DSD accessibility.
CONCLUSION
Digital Smile Design is a significant advancement in aesthetic and prosthetic dental care. The case exemplifies how 3Shape Smile Design Software combined with CAD/CAM fabrication can produce precise, predictable, and highly aesthetic outcomes. Despite challenges related to cost and technical demands, emerging technologies like AI and augmented reality promise to simplify workflows and enhance clinical adoption.

No Files Found




Internationally Accepted
Share Your Publication :