
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Josephat Bakega*, Twisibilege Mwakasungula and Neema Macha
Corresponding Author: Josephat Bakega, Department of Dentistry. Muhimbili National Hospital, Dar-es-salaam, Tanzania.
Received: January 29, 2025 ; Revised: February 01, 2025 ; Accepted: February 04, 2025 ; Available Online: February 17, 2025
Citation: Bakega J, Mwakasungula T & Macha N. (2025) C Nonsurgical Management of Class III Malocclusion with Anterior Open Bite Using the Edgewise Technique: A Case Report and Literature Review. J Oral Health Dent Res, 5(1) 1-5.
Copyrights: ©2025 Bakega J, Mwakasungula T & Macha N. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
Background: Anterior open bite (AOB) is a challenging malocclusion characterized by the absence of vertical overlap between the upper and lower incisors when the mandible is in full occlusion. AOB can be caused by a combination of skeletal, dental, and functional factors, often requiring complex treatment to achieve long-term stability.
Case Presentation: This report discusses an 18-year and 8-month-old male patient presenting with AOB and Class III malocclusion. Clinical examination revealed a 5 mm anterior open bite, 3 mm reverse bite, and mandibular midline deviation of 0.5 mm. Treatment involved fixed orthodontics using the edgewise technique, including first premolar extractions, reverse curve mechanics, box elastics for anterior extrusion, and vertical elastics for open bite correction. After 2.5 years of treatment, the patient achieved Class I canine and incisor relationships, corrected overjet and overbite, improved facial esthetics, and a pleasant smile. A Hawley retainer was provided to prevent relapse.
Conclusion: Successful correction of anterior open bite and Class III malocclusion requires meticulous diagnosis, treatment planning, and a combination of orthodontic techniques. Retention compliance remains critical to minimizing relapse. This case underscores the importance of patient-specific treatment strategies and the challenges of managing vertical malocclusions.
INTRODUCTION
Anterior open bite (AOB) is a challenging malocclusion characterized by a lack of vertical overlap or contact between the upper and lower incisors when the jaw is in full occlusion. It is often associated with a Class III molar relationship, posing significant challenges in orthodontic treatment. AOB is reported to have a prevalence of approximately 3% in adult Caucasian populations but can vary significantly, ranging from 1.5% to 11% across different ethnic groups and age categories [1]. This multifactorial condition often arises from a combination of skeletal, dental, functional, and habitual influences, making it one of the more complex malocclusions to manage [2].
The treatment complexity of AOB lies in its high risk of relapse, regardless of the therapeutic method or retention protocols employed [3]. Achieving stable correction requires a comprehensive approach involving detailed examination, diagnosis, and treatment planning, along with addressing factors such as tongue posture, swallowing habits, and vertical skeletal dimensions. Patient compliance with orthodontic appliances and retainers is critical for achieving long-term stability [4]. This case report details the successful nonsurgical treatment of an 18-year-old male patient with Class III malocclusion and AOB using the edgewise technique, emphasizing the therapeutic approach, treatment outcomes, and a literature-based discussion on the complexities of such cases.
CASE REPORT
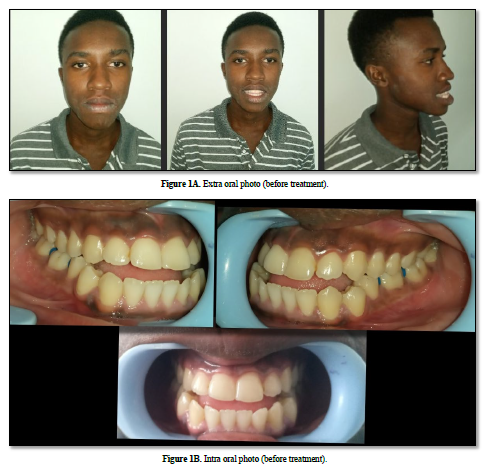
An 18-year-and-8-month-old male patient presented to our orthodontic clinic with complaints of an anterior open bite, difficulty in achieving lip closure, and discomfort during chewing. His past medical and dental histories were unremarkable.
During extraoral examination, the patient exhibited a dolichofacial form, a concave facial profile, and incompetent lips. The nasolabial angle was observed to be within the normal range (Figure 1A). Intraorally, his oral hygiene was average, and gingiva appeared healthy. Occlusal assessment revealed a bilateral Class III molar relationship, Class III canine relationship on both sides, and a Class III incisor relationship. He presented with a 5 mm anterior open bite and a 3 mm reverse overjet (Figure 1B). Additionally, the mandibular dental midline was deviated 0.5 mm to the left. No habits such as thumb-sucking, mouth breathing, or abnormal tongue posture or swallowing were reported.

Treatment Objectives
The treatment objectives included achieving a proper overjet in the sagittal dimension, an ideal anterior overbite in the vertical plane, and coordination of transverse relationships between the maxillary and mandibular arches. Another goal was to improve facial esthetics and restore proper masticatory and articulation functions. Correction of the midline deviation and the creation of a harmonious smile by aligning the smile arc were also prioritized.
Particular emphasis was placed on the vertical reference of the anterior teeth, with the maxillary central incisors' position relative to the lower lip line being a key consideration. Correction of the maxillary and mandibular occlusal planes and axial inclinations of the teeth was planned. This involved molar intrusion and anterior extrusion for vertical correction, guided by the lower facial vertical dimension and anterior esthetic features.
Treatment procedure
The treatment plan included the extraction of mandibular first premolars to resolve the mandibular arch discrepancy and facilitate the correction of the anterior open bite. Conventional brackets were bonded, and the leveling and alignment phase commenced with 0.014” and 0.016” nickel-titanium (NiTi) archwires. This stage achieved initial alignment of both dental arches.
Following leveling, a 0.016” × 0.022” stainless steel archwire was used for mandibular canine retraction and en-masse retraction of the anterior teeth. A reverse curve of Spee was incorporated into the archwire to assist in leveling, while anterior box elastics were prescribed to extrude the anterior teeth and close the open bite. Vertical elastics were applied to stabilize the occlusion and correct midline deviation.
The patient was instructed to wear the elastics for at least 16 hours daily, ensuring consistent application. Regular follow-up appointments were scheduled to monitor compliance and treatment progression. Gradually, the anterior open bite was corrected, and the mandibular midline deviation was resolved. The final phase focused on detailing the occlusion and achieving proper intercuspation. Stabilizing archwires of 0.016” × 0.025” and 0.018” × 0.025” stainless steel was employed.
Treatment outcome
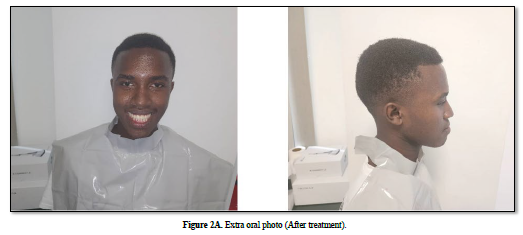
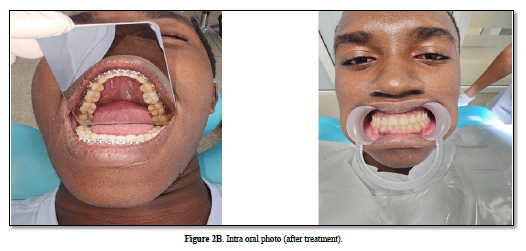
After 2.5 years of treatment, the appliances were removed, and a Hawley retainer was delivered to prevent relapse. Post-treatment evaluation showed that the treatment objectives were successfully achieved. The anterior open bite, overjet, and overbite were corrected, and the mandibular midline deviation was properly aligned (Figures 2A & 2B).
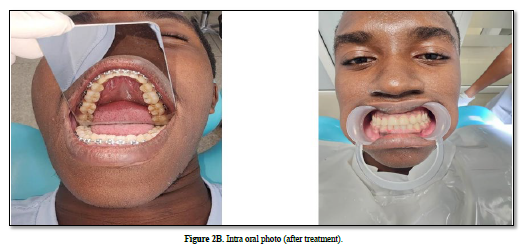
The final occlusion demonstrated a bilateral Class III molar relationship (maintained purposefully), with Class I canine and incisor relationships on both sides. The patient’s facial profile improved from concave to flat, and lip competence was achieved. The smile arc was harmonized, significantly enhancing the patient’s facial esthetics and overall satisfaction.
The patient expressed contentment with the functional and esthetic outcomes, confirming that treatment objectives, including improved masticatory efficiency and facial harmony, were fully met.
LITERATURE REVIEW
Class III malocclusions and AOB pose significant challenges due to their multifactorial etiology and the associated risk of relapse. The etiology of AOB includes a complex interplay of skeletal, dental, and functional factors. Skeletal discrepancies are often related to excessive vertical growth of the maxilla or mandibular overgrowth, while dental components may involve delayed eruption of anterior teeth or intrusion of posterior teeth [5]. Functional factors such as abnormal tongue posture, tongue thrusting, and altered swallowing patterns can further exacerbate the condition [6].
AOB is associated with difficulties in speech, mastication, and esthetics, making timely and effective management crucial [7]. Nonsurgical treatment of Class III malocclusion with AOB typically involves fixed appliances combined with elastics and auxiliary mechanics. Studies emphasize the importance of correcting the vertical dimension by modifying occlusal planes and addressing the axial inclinations of the anterior and posterior teeth [8]. Intrusion of posterior teeth and extrusion of anterior teeth are commonly employed mechanics for vertical correction. However, maintaining the vertical stability of the corrected occlusion is a significant challenge, with relapse rates reported to be as high as 30% in some studies [9].
Retention is critical in preventing relapse following active treatment. Removable retainers, such as Hawley retainers, are widely used, but their effectiveness depends heavily on patient compliance. The literature underscores the importance of addressing the underlying etiological factors, such as tongue posture and habits, to achieve stable outcomes [10].
DISCUSSION
The treatment of AOB and Class III malocclusion is often considered one of the most challenging aspects of orthodontics due to the high risk of relapse and the complex mechanics required for correction. This case highlights the importance of a detailed diagnosis and tailored treatment plan in achieving stable outcomes. The extraction of mandibular premolars in this case facilitated en-masse retraction and helped achieve proper overjet and overbite relationships without surgical intervention. The use of box and vertical elastics proved effective in correcting the anterior open bite by extruding the anterior teeth and stabilizing the occlusion.
One of the key factors contributing to the success of this treatment was the patient’s compliance with elastic wear and retainer use. Studies indicate that compliance is a critical determinant of long-term stability in nonsurgical AOB correction [11]. Additionally, the incorporation of finishing mechanics ensured proper intercuspation and occlusal stability. The patient’s post-treatment facial esthetics and functional outcomes were markedly improved, aligning with findings in the literature that emphasize the psychosocial benefits of addressing open bite malocclusion [12,13].
Despite the favorable outcome, the risk of relapse remains a concern. Relapse in AOB cases is often attributed to insufficient retention, lack of habit control, or failure to address skeletal discrepancies during treatment. Future follow-ups will be crucial to monitor stability and ensure the patient’s adherence to the retention protocol [14].
CONCLUSION
The successful nonsurgical correction of Class III malocclusion with anterior open bite in this case underscores the effectiveness of the edgewise technique combined with proper mechanics and patient compliance. Detailed diagnosis, individualized treatment planning, and regular follow-ups were essential to achieving the desired outcomes. While the results were stable at the end of active treatment, long-term retention and monitoring remain critical to minimizing the risk of relapse. This case reinforces the importance of addressing both functional and esthetic concerns in orthodontic treatment to improve patient quality of life.

No Files Found




Internationally Accepted
Share Your Publication :