
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Azita Azad, Jannan Ghapanchi, Fahimeh Rezazadeh, Abdolaziz Haghnegahdar, Azita Sadeghzadeh, Armaghan Tarjan and Zahra Mansouri*
Corresponding Author: Zahra Mansouri, Oral and Dental Disease Research Center, Department of Oral and Maxillofacial Medicine, School of Dentistry, Shiraz University of Medical Sciences, Shiraz, Iran.
Received: June 09, 2024 ; Revised: June 17, 2024 ; Accepted: June 20, 2024 ; Available Online: August 14, 2024
Citation: Azad A, Ghapanchi J, Rezazadeh F, Haghnegahdar A, Sadeghzadeh A, et al. (2024) Frequency of Tonsilloliths in the Panoramic Radiographs of Patients Who are Candidates for Kidney Transplant: A Cross-Sectional Study in Shiraz, South of Iran-The Incidence of Tonsillolith in ESRD. J Oral Health Dent Res, 4(1): 1-4.
Copyrights: ©2024 Azad A, Ghapanchi J, Rezazadeh F, Haghnegahdar A, Sadeghzadeh A, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
Introduction: As dystrophic calcifications, tonsilloliths are calcified compositions located in enlarged tonsillar crypts. These stones may be more prevalent in some systemic diseases such as chronic kidney disease (CKD) due to osteodistrophic changes.
Objectives: The aim of this survey was evaluating the prevalence of tonsillar stones in the panoramic radiographs of CKD compared to healthy subjects.
Patients and Methods: In this cross-sectional study, 140 panoramic views of CKD patients who were candidates for kidney transplant and 140 healthy individuals were included. The images were observed on a Barco monitor (China) in a semi-darkened room and evaluated by two calibrated oral radiologists and post graduate students.
Results: In CKD group, three cases (16.6%) had right side, nine (50%) had left side, and six (33.3%) had tonsilloliths on both sides. Four cases (2.85%) of kidney transplant group also had both tonsillar stones and calcified stylohyoid ligament. In normal group, four (57%) of the subjects had both sides, two (28.5%) had right side and one (14.2%) had left side stones. All of the lith sizes were estimated smaller than 5 mm, and most were diagnosed as 2-7 oval, round or irregular particles in shape.
Conclusion: This study result showed that tonsilloliths were more prevalent on panoramic radiographs of kidney transplant cases. Dentists should be familiar with these entities and their oral manifestations.
Keywords: Tonsilloliths, Panoramic radiograph, Kidney transplant, Chronic kidney disorder
Implication for health policy/practice/research/medical education: Tonsilloliths are calcified compositions located in enlarged tonsillar crypts that may be more prevalent in chronic kidney disease (CKD) due to osteodistrophic changes. This study result showed that tonsilloliths were more prevalent on panoramic radiographs of kidney transplant cases. Dentists should be familiar with these entities and their oral manifestations.
INTRODUCTION
Tonsilloliths, also called tonsil stones or tonsillar concretions, are infrequent calcified compositions located in extended adenoidal crypts due to an uncommon structure of dystrophic calcification.
Tonsilloliths commonly appear as several small and ill-defined radiopacities located on the ramus [1]. These calcifications are made from calcium salts such as hydroxyapatite or calcium carbonate apatite, oxalates, and other magnesium salts and ammonium radicals. Calcium is placed on desquamated epithelial cells and accompanied by the accumulation of bacteria in the palatine tonsils or crypts. They may or may not be associated with tonsillitis so they are normally small with unknown etiology [2,3]. Many studies have reported that these structures might be associated with lithiasis in some other parts of the body [4]. Nearby, a large number of tonsilloliths are symptomless, but huge palatine tonsilloliths may cause periodic or sustained irritation of the throat, cough, soreness, discomfort, dysphagia, foreign body sensation, oral malodor, taste changes, ear pain, enlarged neck glands tenderness, a lump in the throat, peritonsillar abscess, trismus, neuralgia of the glossopharyngeal nerve and pain in the orofacial area [5]. These symptoms may be discovered in panoramic or lateral cephalometric images [6]. Differentiating tonsilloliths from various opacities of the jaws may be challenging particularly in asymptomatic cases. Many disorders such as cancers, calcification in the lymph node and salivary gland, phleboliths, calcified granulomas, and scrofula fall under the differential diagnosis of such lesions [7]. Inadequate diagnosis may trigger emotional stress and improper treatment for the patient. Awareness of the physician regarding the location, prevalence, anatomical diversity, radiographic appearance, normal size, and count of tonsilloliths is highly conducive and cost effective. In orthopantomography images, tonsillitis looks like solitary or numerous radiopaque lesions on the ramus in a region where the dorsal surface of the tongue crosses it in the palatoglossal or glossopharyngeal air spaces [7].
Chronic kidney disease (CKD) is a major cause of mortality and morbidity in the world.
All CKD cases undergo panoramic radiography prior to transplant in order to identify any cause of infection in the mouth. This radiography is low-cost, widely used, and simple, entailing a low dose of irradiation [8]. Moreover, its use in evaluating tonsilloliths has previously been documented [6]. As stated earlier, tonsilloliths may cause variable symptoms in mouth, jaw, and face in unfamiliar to numerous dentists and physician. To the best of our knowledge, there is no documented evidence as to the presence of tonsillar calcifications in CKD cases.
OBJECTIVES
This study was conducted to assess the prevalence of tonsillar stones in the panoramic radiographs of CKD cases compared to healthy subjects.
PATIENTS AND METHODS
In this cross-sectional study, 140 panoramic views of CKD patients (66 females, 74 males, 16-70 years old) who were candidates for kidney transplant and 140 healthy individuals (70 females, 70 males, aged 15-68 years) were included. All participants were referred to Shiraz University Dental Clinic (Shiraz Dental School, Shiraz, Iran) for a pre-transplant oral examination. A control group was also randomly selected from healthy individuals attending the same clinic for routine dental care between May 2017 and July 2019. Written informed consent was obtained from each participant. Afterwards, subjects with acceptable quality panoramic radiographs were included. Cases with a history of tonsillectomy were excluded from the study. The collected demographic data included gender, age, and disease duration.
Panoramic radiographs were prepared using a Planmeca XC Proline panoramic machine (Helsinki, Finland). Using Agfa PSP receptors (Germany), exposure factors were adjusted according to the size and age of the patient (57-85 kVp, 10 mA). The images were observed on a Barco monitor (China) in a semi-darkened room.
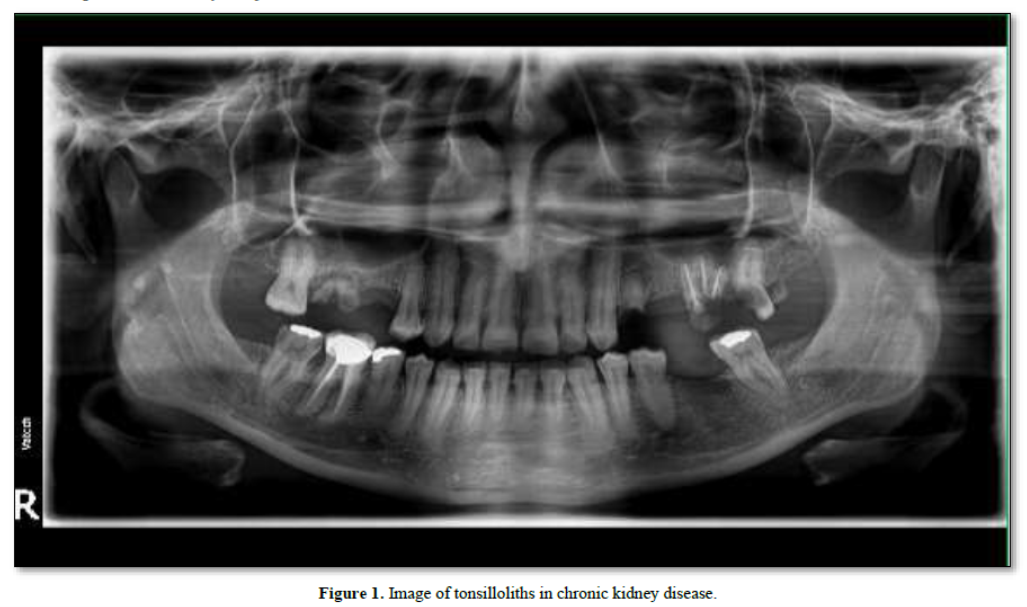
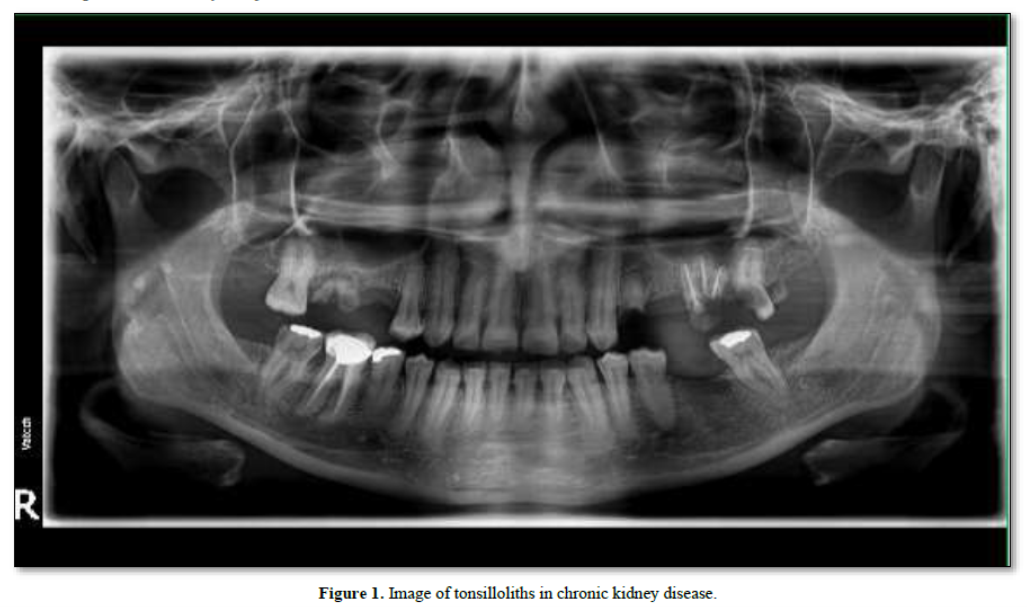
The presence of tonsillar calculi was investigated on panoramic radiographs by two calibrated oral radiologists and a post graduate student based on reported criteria by Takashi [9]. According to this definition, tonsilloliths are numerous small and ill-defined radiopacities located on the ramus or the masses were gathered on the mandible and soft palate and frequently superimposed over the border of the tongue shadow (Figure 1).
Since the radiographs were taken for other dental purposes, no extra dose was exposed to the patients; therefore, there was no ethical limitation to conducting the study.
ETHICAL CONSIDERATIONS
The research followed the tents of the Declaration of Helsinki. The Ethics Committee of Shiraz University of Medical Sciences approved this study. The institutional ethical committee at shiraz University of Medical Sciences approved all study protocols N(IR.SUMS.MED.REC.1399.177). Accordingly, written informed consent taken from all participants before any intervention. This study was extracted from undergraduate thesis of Sara Pourshahid at this university (Thesis#22049).
STATISTICAL ANALYSIS
Data were analyzed to detect the frequency and percentage of liths in both groups by SPSS version 17 (SPSS Inc., Chicago, Il, USA). Chi-square test, odds ratio (OR), and 95% confidence interval (95% C.I) were considered to assess the association between liths and groups. P< 0.05 was considered as statistically significant.
RESULTS
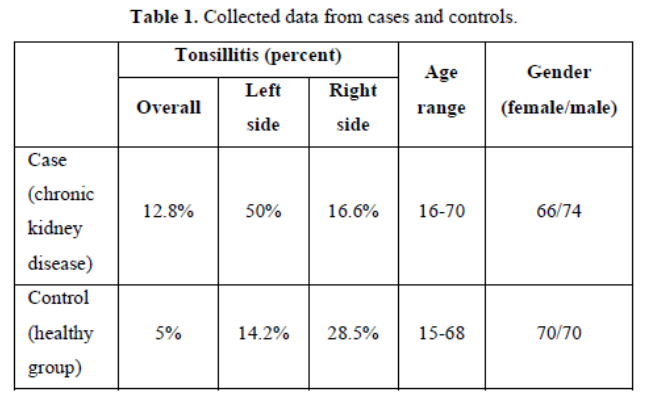
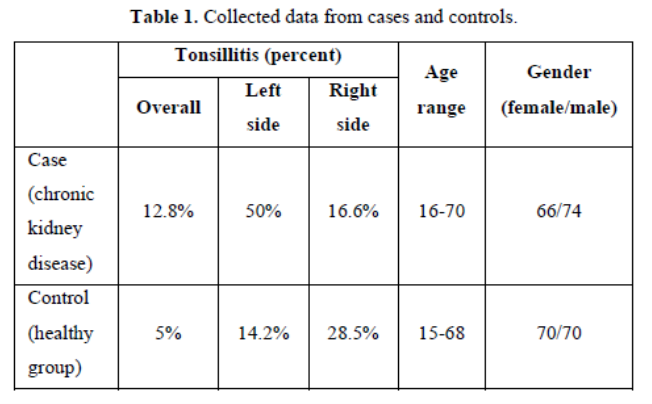
Out of the 140 CKD individuals, 18 (12.8%) (11 females and 7 males) had tonsilloliths on panoramic radiographs. In the controls, 7(5%) (six females and one male) had calcification. Statistical analysis showed that CKD patients were 2.8 times more likely to have tonsilliths compared to healthy subjects (OR=2.8, 95% CI=1.13-6.94. p=0.021).
In CKD group, three (16.6%) of the cases had right side, nine (50%) had left side, and six (33.3%) had tonsilloliths both sides. Four cases (2.85%) of kidney transplant group also had both tonsillar stones and calcified stylohyoid ligament.
In the normal group, four (57%) of the subjects had both sides, two (28.5%) had right side and one (14.2%) had left side stones. All liths were estimated to be smaller than 5 mm, and most were diagnosed as 2-7 oval, round or irregular particles in shape (Table 1).
DISCUSSION
Soft tissue calcifications are commonly observed in end stage renal failure due to calcium and phosphate imbalance and concomitant hyperparathyroidism [10]. Extraosseous calcification entails myriad problems in hemodialysis cases [11].
Calcium deposition occurs more often in the first- and second-year following treatment. The causes of calcium deposition are the plasma calcium-phosphorus level, nonoptimal calcium and magnesium ion concentration in the dialysis bath, and parathyroid hyperfunction [12]. As an obvious finding in chronic renal failure, hyperphosphatemia induces extraosseous calcifications of soft tissues [11].
Soft tissue calcifications are generally asymptomatic and frequently found incidentally. The localization and diagnosis of such lesions in the head and neck are problematic because the structures are close to each other; moreover, it is hard to differentiate the radiopacity situated either in the jawbone or mucosa owing to the superimpositions [13].
Rhinolith, antrolith, phlebolith, tonsillolith, arteriosclerotic plaque, and arteriosclerosis comprise a major part of head and neck dystrophic calcification [14]. In spite of the standard serum and calcium phosphate measure, dystrophic calcifications are mentioned as pathological; furthermore, they are diagnosed in degenerative or reduced tissues induced by trauma, irritation, microorganisms (parasites), injections, and systemic diseases [13].
Soft tissue calcification of the maxillofacial area is rare and typically noticed during routine screening radiographs. Anatomical site, scattering, amount, dimensions, and form of the calcifications are the key diagnostic factors for their identification [14,15].
In the current research, we evaluated the prevalence of tonsilloliths in a selected community and observed that tonsillar stones were more prevalent in CKD cases compared with the normal group. More accurate diagnosis of tonsilloliths can be established by clinical symptoms, intraoral checkup, and imaging [3,16].
On panoramic radiographs, these calcifications might not be distinguished from other calcified lesions such as calcification or elongation of stylohyoid process, tooth, foreign objects, sialoliths, phleboliths, or lymph node calcification [6,17].
Imaging can help physicians identify the precise measurement, extension, and location of the particles(8). Tonsillectomy is used to treat the symptomatic or huge tonsilloliths [18].
In this study, we used orthopantomography, and screening method used in most dental procedures as an easy-access imaging method with low-dose irradiation [19].
CBCT is a valuable and accurate modality for better diagnosis. However, due to its higher required doses of irradiation and high cost, we were not able to use this imaging method for such epidemiologic research [6].
Review of literature presented that the prevalence of tonsilloliths was under 25% [17]. A study in Shiraz showed that the rate of tonsilloliths was 5.05% of general population [6]. In this study, CRF cases had a higher rate (12.8%) of tonsillar concretion compared with previous studies [6]. This may be related to a calcium-phosphor imbalance which could lead to soft tissue calcification.
CONCLUSION
This study result showed that tonsilloliths could be seen incidentally on panoramic radiographs taken for dental treatment especially in kidney transplant cases. Physicians should be familiar with these entities and differentiate them from other radiopaque lesions.
LIMITATIONS OF THE STUDY
It should be noted that we did not have the previous pantomo graphs of either group to evaluate the existence of the lesions. Therefore, we were not able to precisely determine whether the lesions were related to kidney disease or not. A longitudinal study on a specific and larger group is necessary for more accurate results.
It should be further noted that in this cross-sectional research, we had a limited time and could only observe the soft tissue lesions at the examination period.
No Files Found




Internationally Accepted
Share Your Publication :