
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Ani Simila CS*, Raghu Dhanapal, Dinakar, Jaishlal and Gomakumar
Corresponding Author: Dr. C.S. Ani Simila MDS, Senior lecturer, Department of Oral and maxillofacial pathology and Oral Microbiology, Rajas Dental College and Hospital, Vadakankulam, Thirunelveli -627105.Kanyakumari, Tamil Nadu, India.
Received: March 02, 2024 ; Revised: March 14, 2024 ; Accepted: March 17, 2024 ; Available Online: April 02, 2024
Citation: Simila ACS, Dhanapal R, Dinakar, Jaishlal & Gomakumar. (2024) Monophasic Fibrous Synovial Sarcoma of Oral Cavity - A Rare Case Report. J Oral Health Dent Res, 4(1): 1-6.
Copyrights: ©2024 Simila ACS, Dhanapal R, Dinakar, Jaishlal & Gomakumar. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
Background: Synovial sarcoma is a rare malignant mesenchymal neoplasm of unknown etiology accounting for 1.9%-3.7% in the oral cavity. More commonly it is seen in the soft tissues of lower extremities. It is a rare phenomenon of occurrence in the oral cavity.
Case presentation: A 31-year-old female patient presented with the painful swelling in the left lower back tooth region for two months. The histopathological examination revealed a monophasic fibrous synovial sarcoma. Immunohistochemical findings showed strong positivity for CD99, Bcl2 and negative for CD34 confirmed the diagnosis of synovial sarcoma.
Conclusion: Occurrence of synovial sarcoma in the oral cavity is extremely rare. Advanced molecular diagnostic techniques are needed for rapid and definitive diagnosis.
Keywords: Synovial sarcoma, Mesenchymal, Monophasic, Molecular
INTRODUCTION
Synovial sarcoma (SS) is a malignant mesenchymal tumor of rare entity [1]. Synovial Sarcoma is a misnomer as it is not related to synovium or synovial membrane [2,3]. They are named as SS for resembling the histological appearance of the synovium [3,4]. SS is a rare tumor of erratic histogenesis but it is believed to arise from the pluripotential mesenchymal cells [4]. The occurrence of SS in the head and neck region range from 5.6%-10% [5].
The most common primary sites of synovial sarcoma are the lower extremities, especially the joint capsules, knees, tendon sheaths and bursae [6]. Oral SS accounts for 1.9%-3.7% with high incidences in the hypopharynx, parapharyngeal region and parapharyngeal space [5]. Literature reviews showed that the SS is seen in the third decades with slight male predilection. Occurrence of SS in the oral cavity is an extremely rare condition with only 31 intraoral cases have been reported so far [1,5]. It is often misdiagnosed because of the unusual location [5]. Here with reporting a case of SS of the retromolar region in a 31-year-old female which was previously diagnosed as solitary fibrous tumors.
CASE REPORT
A31-year-old female patient presented with the chief complaint of painful swelling in the lower left back tooth region for two months. The pain was of sudden onset, continuous in nature and increased on mastication. The patient was moderately built and poorly nourished. All the vital signs are within the physiological limits. Extra orally, facial asymmetry with a swelling on left side of size 2×2 cm. Antero posteriorly, it extends from 3cm behind the corner of the lip to the angle of the mouth. Superioinferiorly, from the line joining the corner of the lip to the tragus of the ear to the lower border of the mandible. The nasolabial fold is stretched and the patient felt pain while opening and closing the jaw. The overlying skin was smooth with no discharge. The mass was hard, tender and warm on palpation. Intraorally, the swelling extends from 37 to the retromolar region. Surface was smooth with no ulcerations (Figure 1).

Complete blood investigations revealed an elevated lymphocytic count and elevated ESR. OPG examination showed an ill-defined radiolucency in the retromolar region of 3x3 cm in size, involving the inferior alveolar canal (Figure 2).

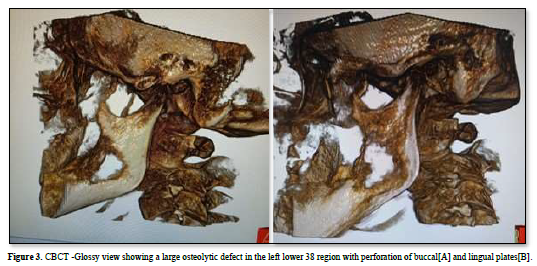
CT scan revealed a large osteolytic defect of size 3× 3 cm in the 38-region extending till the anterior border of the ramus with perforation of lingual & buccal plates (Figure 3).

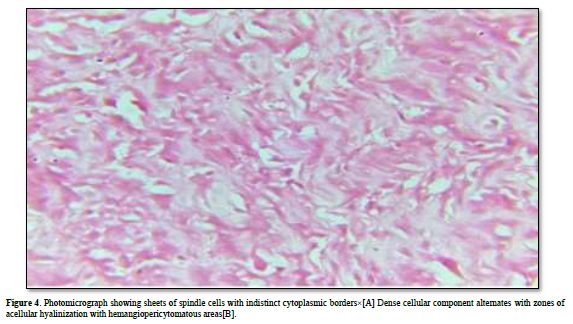
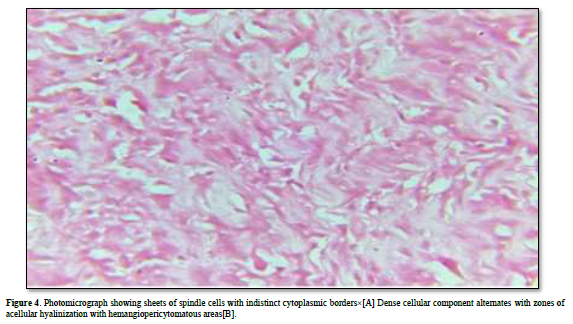
An incisional biopsy was performed under local anesthesia and submitted for histopathological examination. Hematoxylin and eosin-stained soft tissue section revealed pattern-less arrangement of spindle cells in a collagenous background with a prominent vascularity that results in a hemangiopericytoma-like pattern. Therefore, an interim diagnosis of solitary fibrous tumor was made based on the characteristic microscopic appearance. Subsequently, an excisional biopsy was done as the pain persists. Histopathological examination revealed sheets of spindle cells with focal areas of interspersed epithelioid cells. The spindle cells were plump shaped with indistinct cytoplasmic borders. Dense cellular component alternates with zones of acellular hyalinization. Cellular atypia was minimal. Mitotic figures were absent. Vascularity was moderate exhibiting hemangiopericytoma like areas and perivascular hyalinization of blood vessels. Differential diagnosis of hemangiopericytoma, fibrosarcoma and malignant fibrous histiocytoma was made (Figure 4).
Special stain like periodic acid Schiff stain was found to be negative indicating that these hyaline deposits are mesenchymal mucins secreted by the malignant spindle cells.
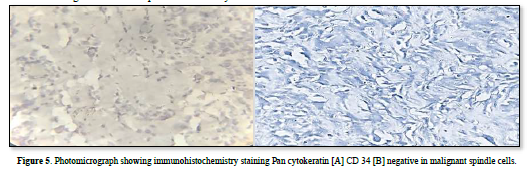
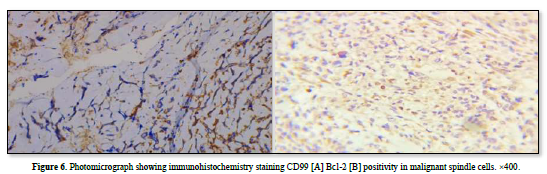
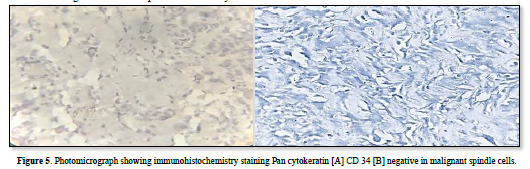
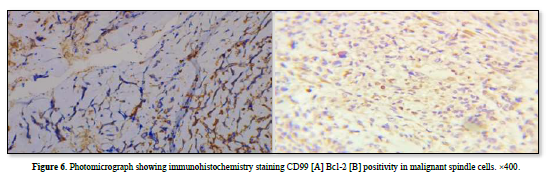
Immunohistochemistry showed strong positivity for CD99, Bcl-2and negative CD34, pan cytokeratin confirmed the diagnosis of monophasic fibrous synovial sarcoma. These results were consistent to the histopathological diagnosis (Figures 5 & 6).
The patient was referred to higher medical center for further management. The patient expired within three months as she neglected the treatment.
DISCUSSION
Synovial sarcoma was first defined by Simon in 1865 [7] and was labelled as SS by Sabrazes in 1934 [8]. The etiopathogenesis and the histogenesis of SS is undefined but thought to be originated from the mesenchymal pluripotential cells. They are labelled as SS as it resembles to the histological features of synovium or synovial membrane [9]. About 90-95% of SS revealed consistent, specific reciprocal translocation, t (X:18) (p11.2-q11.2) that forms the fusion of SYT with either SSXI or SSX2 gene. The most common cytogenetic findings in monophasic fibrous tumor SYT: SSX2 whereas biphasic tumor demonstrates the fusion of SYT: SSX1[10,11]. The SS is mainly mediated by the Wnt/β- catenin, ERK and PcG signaling pathways [12]. In addition, EMT signaling pathway is also implicated in the molecular pathogenesis of SS [13].
Head and neck synovial sarcoma accounts for 5-10% of total sarcomas whereas occurrence of oral SS is 1.9%-3.7% [5]. SS is more commonly seen in the adolescents and young age group with a mean age of 15-40 years with a slight male predilection [14,15]. Palpable deep-seated swelling with mild pain or tenderness is the common clinical manifestation of SS [10]. Early stages of SS present with an indolent swelling, upsurges over months to years, varying in sizes from 2-3 cms to 10-14 cms. Initial stages may mimic as benign lesion [16]. About 85-95% SS is predominantly seen in the lower extremities intimately associated with the tendon and tendon sheaths, knees, large joints and bursae [14]. Para vertebral space is the second most common site of SS and manifest as solitary masses in the retropharyngeal or parapharyngeal region [10]. Oral SS manifest as minor limitation of movement, hoarseness, numbness of the lip, dysphagia [16]. Because of the unusual location, it is often misdiagnosed. In the present case, initially it was misdiagnosed as solitary fibrous tumor due to insufficient tissue specimen and of the rarity of oral SS.
Histologically, SS is classified into four sub types: biphasic, monophasic fibrous type predominantly consists of spindle cells, monophasic epithelioid cells and poorly differentiated tumors [10]. The monophasic fibrous type exhibits sheets of well oriented spindle cells having indistinct cytoplasm alternating with less cellular areas of hyalinization. The perivascular hyalinization and thick collagen bands separating the malignant spindle cells is the striking feature of monophasic fibrous type [10]. The reported case exhibits sheets of spindles with unclear cytoplasmic borders alternating with dense areas of hyalinization and perivascular hyalinization. Hemangiopericytoma, fibrosarcoma, malignant fibrous histiocytoma and leiomyosarcoma are considered as the differential diagnosis of this lesion. Periodic acid Schiff (PAS) stain was found to be negative as these hyalinized areas are stromal or mesenchymal mucins secreted by the malignant spindle cells. Immunohistochemical evaluation showed that tumor cells expressed CD 99 and 70% positivity of Bcl-2. CD34 and pancytokeratin were found to be negative in this case. A positive pancytokeratin antibody aids in separating sarcomas from carcinomas and epithelial tissues [17]. Because mucosal melanoma and malignant spindle cell carcinoma are epithelial in origin, these tumors were ruled out in this case by the negative pancytokeratin test. In some cases, uncertain histopathological features or mystifying immunohistochemical results, RT-PCR or FISH helps to diagnose oral SS. [18,19]. The specificity and sensitivity of RT-PCR test was approximately 83.8% and Fluorescent in situ hybridization (FISH) was 80% and the collective detection rate of both was 92.9% [20].
Most reviewers pointed out that SS is a chemo sensitive sarcoma but radical local excision with adjunctive radiotherapy is recommended to be the successful treatment for Oral SS [10]. Oral SS most commonly metastasis to lung, bone marrow and lymph nodes [5]. High grade malignant SS has a recurrence rate of 80% whereas the recurrence rate of oral SS is 20.8% [6].
The prognosis (5-year survival rate) for high grade SS is found to be 64-76% and in oral SS it is about 55% [21]. In addition, the prognosis is poor if the margins are inadequately cleared, without any adjunctive therapy, age, size and location of the tumor, high grade staging and metastasis [13].
The favorable clinical outcome of the patient includes clear surgical margin minimal cellular atypia, less than 5/10 HPF and presence of calcifications [2]. Calcifications is always preceded by hyalinization. Extensively calcified SS has a good long-term prognosis. The median survival rate in case of extensively calcified SS was about 80% and in monophasic fibrous synovial sarcoma was about 50% [10]. In the present case, patient had a poor prognosis as the patient neglected the treatment.
CONCLUSION
The term "synovial sarcoma" is thought to be misleading because it develops in areas where there aren't any typical synovial structures. Because of its odd location and rarity, oral SS is frequently misdiagnosed. For a precise diagnosis of oral synovial sarcoma, advanced molecular techniques including fluorescent in situ hybridization (FISH) and reverse transcription-polymerase chain reaction (RT-PCR) are required. When conventional approaches are ineffective for diagnosing oral synovial sarcoma, the identification of SYT-SSX2 fusion transcript by RT-PCR is an important diagnostic tool.



No Files Found




Internationally Accepted
Share Your Publication :